Department of Pediatrics, Kobe University Graduate School of Medicine, 7-5-2 Kusunoki-cho, Chuo-ku, Kobe, Hyogo, 650-0017, Japan.
Department of Neurology, Hyogo Prefectural Kobe Children's Hospital, 1-6-7 Minatojima-minamimachi, Chuo-ku, Kobe, Hyogo, 650-0047, Japan.
BMC Neurol. 2022 Mar 5;22(1):77. doi: 10.1186/s12883-022-02608-2.
Febrile status epilepticus is the most common form of status epilepticus in children. No previous reports compare the effectiveness of treatment strategies using fosphenytoin (fPHT) or phenobarbital (PB) and those using anesthetics as second-line anti-seizure medication for benzodiazepine-resistant convulsive status epilepticus (CSE). We aimed to examine the outcomes of various treatment strategies for febrile convulsive status epilepticus (FCSE) in a real-world setting while comparing the effects of different treatment protocols and their presence or absence.
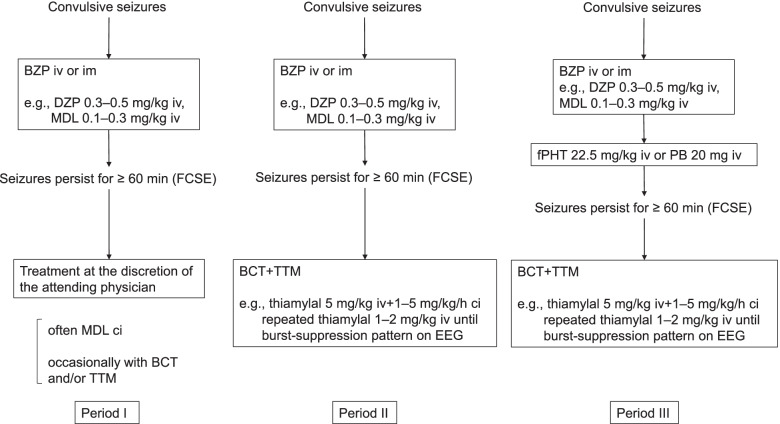
This was a single-center historical cohort study that was divided into three periods. Patients who presented with febrile convulsive status epilepticus for ≥60 min even after the administration of at least one anticonvulsant were included. During period I (October 2002-December 2006), treatment was performed at the discretion of the attending physician, without a protocol. During period II (January 2007-February 2013), barbiturate coma therapy (BCT) was indicated for FCSE resistant to benzodiazepines. During period III (March 2013-April 2016), BCT was indicated for FCSE resistant to fPHT or PB.
The rate of electroencephalogram monitoring was lower in period I than period II+III (11.5% vs. 85.7%, p<0.01). Midazolam was administered by continuous infusion more often in period I than period II+III (84.6% vs. 25.0%, p<0.01), whereas fPHT was administered less often in period I than period II+III (0% vs. 27.4%, p<0.01). The rate of poor outcome, which was determined using the Pediatric Cerebral Performance Category scale, was higher in period I than period II+III (23.1% vs. 7.1%, p=0.03). The rate of poor outcome did not differ between periods II and III (4.2% vs. 11.1%, p=0.40).
While the presence of a treatment protocol for FCSE in children may improve outcomes, a treatment protocol using fPHT or PB may not be associated with better outcomes.
发热性癫痫持续状态是儿童中最常见的癫痫持续状态形式。以前没有报告比较使用苯妥英(fPHT)或苯巴比妥(PB)的治疗策略与使用麻醉剂作为苯二氮䓬类耐药惊厥性癫痫持续状态(CSE)的二线抗癫痫药物的疗效。我们旨在检查在真实环境中各种治疗策略对发热性惊厥性癫痫持续状态(FCSE)的结果,同时比较不同治疗方案的效果及其存在或不存在。
这是一项单中心历史队列研究,分为三个时期。纳入至少使用一种抗惊厥药物后仍持续 60 分钟以上的发热性惊厥性癫痫持续状态患者。在第一期(2002 年 10 月至 2006 年 12 月),治疗由主治医生自行决定,没有方案。在第二期(2007 年 1 月至 2013 年 2 月),对于苯二氮䓬类耐药的 FCSE,指示进行巴比妥酸盐昏迷疗法(BCT)。在第三期(2013 年 3 月至 2016 年 4 月),对于 fPHT 或 PB 耐药的 FCSE,指示进行 BCT。
第一期脑电图监测率低于第二期和第三期(11.5% vs. 85.7%,p<0.01)。咪达唑仑在第一期更常通过连续输注给予,而在第二期和第三期则较少(84.6% vs. 25.0%,p<0.01),而在第一期给予 fPHT 则较少(0% vs. 27.4%,p<0.01)。使用小儿脑功能分类量表确定的不良预后率在第一期高于第二期和第三期(23.1% vs. 7.1%,p=0.03)。第二期和第三期的不良预后率没有差异(4.2% vs. 11.1%,p=0.40)。
虽然儿童 FCSE 治疗方案的存在可能改善预后,但使用 fPHT 或 PB 的治疗方案可能不会带来更好的预后。