Herbert Irving Comprehensive Cancer Center, Columbia University Irving Medical Center, New York, NY.
Department of Medical Oncology, Mount Vernon Cancer Centre, London, United Kingdom.
J Clin Oncol. 2022 Jun 10;40(17):1939-1948. doi: 10.1200/JCO.21.01805. Epub 2022 Mar 7.
This phase I study aimed to define the recommended phase II dose (RP2D) of tebentafusp, a first-in-class T-cell receptor/anti-CD3 bispecific protein, using a three-week step-up dosing regimen, and to assess its safety, pharmacokinetics, pharmacodynamics, and preliminary clinical activity in patients with metastatic uveal melanoma (mUM).
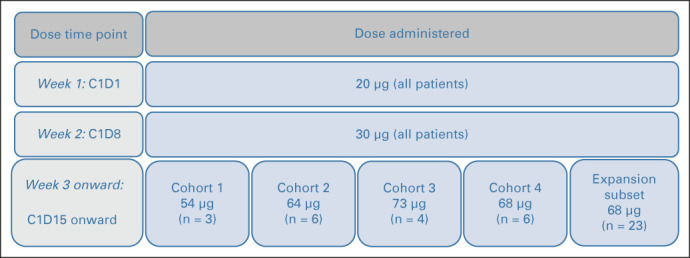
In this open-label, international, phase I/II study, HLA-A02 or HLA-A02:01+ patients with mUM received tebentafusp 20 μg once in week 1 and 30 μg once in week 2. Dose escalation (starting at 54 μg) began at week 3 in a standard 3 + 3 design to define RP2D. Expansion-phase patients were treated at the RP2D (20-30-68 μg). Blood and tumor samples were collected for pharmacokinetics/pharmacodynamics assessment, and treatment efficacy was evaluated for all patients with baseline efficacy data as of December 2017.
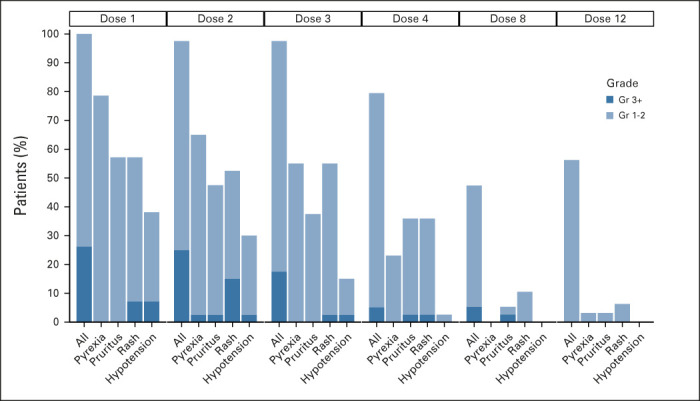
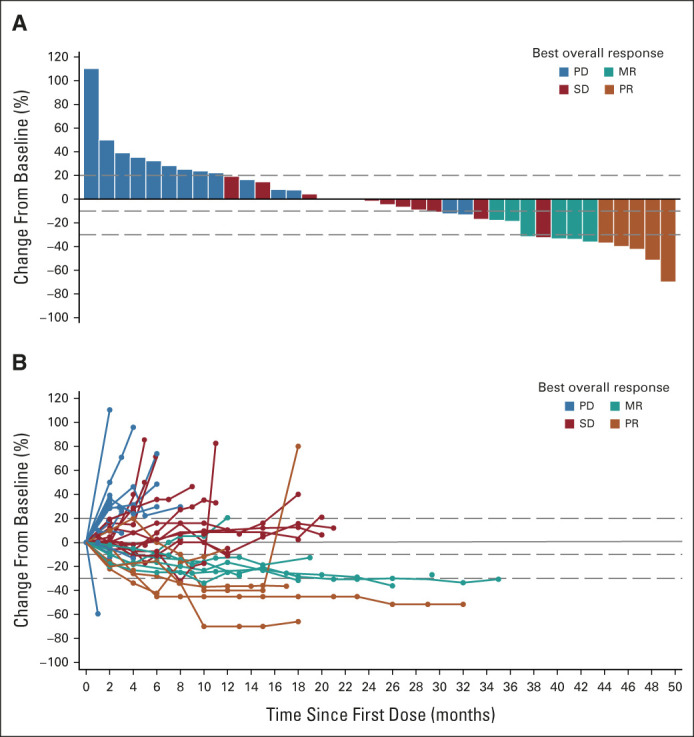
Between March 2016 and December 2017, 42 eligible patients who failed a median of two previous treatments were enrolled: 19 in the dose escalation cohort and 23 in an initial dose expansion cohort. Of the dose levels investigated, 68 μg was identified as the RP2D. Most frequent treatment-emergent adverse events regardless of attribution were pyrexia (91%), rash (83%), pruritus (83%), nausea (74%), fatigue (71%), and chills (69%). Toxicity attenuated following the first three doses. The overall response rate was 11.9% (95% CI, 4.0 to 25.6). With a median follow-up of 32.4 months, median overall survival was 25.5 months (range, 0.89-31.1 months) and 1-year overall survival rate was 67%. Treatment was associated with increased tumor T-cell infiltration and transient increases in serum inflammatory mediators.
Using a step-up dosing regimen of tebentafusp allowed a 36% increase in the RP2D compared with weekly fixed dosing, with a manageable side-effect profile and a signal of efficacy in mUM.
本 I 期研究旨在采用三周递升剂量方案确定新型 TCR/抗 CD3 双特异性蛋白替本福司(tebentafusp)的 II 期推荐剂量(RP2D),并评估其在转移性葡萄膜黑色素瘤(mUM)患者中的安全性、药代动力学、药效学和初步临床活性。
在这项开放标签、国际 I/II 期研究中,HLA-A02 或 HLA-A02:01+的 mUM 患者接受替本福司 20μg,第 1 周和第 3 周各一次,第 2 周 30μg 一次。从第 3 周开始,采用标准的 3+3 设计进行剂量递增,以确定 RP2D。扩展阶段患者按照 RP2D(20-30-68μg)治疗。采集血样和肿瘤样本进行药代动力学/药效学评估,所有基线时具有疗效数据的患者均进行治疗效果评估,截至 2017 年 12 月。
2016 年 3 月至 2017 年 12 月,共纳入 42 例符合条件的既往治疗失败中位数达 2 次的患者:19 例入剂量递增队列,23 例入初始剂量扩展队列。在研究的各剂量水平中,确定 68μg 为 RP2D。无论病因如何,最常见的治疗相关不良事件为发热(91%)、皮疹(83%)、瘙痒(83%)、恶心(74%)、乏力(71%)和寒战(69%)。在前 3 剂后毒性减轻。总体缓解率为 11.9%(95%CI,4.0 至 25.6)。中位随访 32.4 个月时,中位总生存期为 25.5 个月(范围:0.89 至 31.1 个月),1 年总生存率为 67%。治疗与肿瘤 T 细胞浸润增加和血清炎症介质的短暂升高相关。
采用递升剂量方案给予替本福司,与每周固定剂量相比,RP2D 增加了 36%,具有可管理的副作用谱和 mUM 患者的疗效信号。