Kıhtır Hasan Serdar, Akçay Nihal, Şevketoğlu Esra
Department of Pediatric Critical Care, University of Health Sciences Antalya Training and Research Hospital, Antalya, Turkey.
Department of Pediatric Critical Care, University of Health Sciences Bakırköy Dr. Sadi Konuk Training and Research Hospital, İstanbul, Turkey.
Turk J Anaesthesiol Reanim. 2022 Feb;50(1):18-23. doi: 10.5152/TJAR.2021.1412.
The objective of this study is to present our experience using the pressure-regulated volume control and the pressure-control ventilation modes in children.
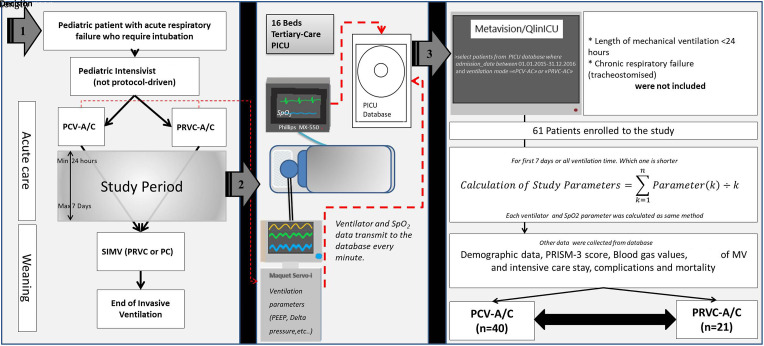
Patients with acute respiratory failure ventilated with pressure-regulated volume control or pressure-control modes were retrospectively evaluated. The patient's ventilation parameters (of the first 7 days of ventilation or of the whole ventilation period, if the patient had been ventilated less than 7 days), SpO2, blood gases, and demographic data were collected from the pediatric intensive care unit database.
Sixty-one patients (median age 12 [4.8-36.4] months) were enrolled in the study. The pressure-control ventilation mode was used on 40 patients (65.6%) and the pressure-regulated volume-control mode was used on 21 (34.4%) patients. Twenty-eight patients (45.9%) had hypoxemic respiratory failure and 44 (72.1%) had hypercapnic respiratory failure. The median positive end-expiratory pressure was higher in pressure-control ventilation mode (5.4 [4.2-6.3] cmH2O) than the pressure-regulated volume-control mode (4.05 [3.68-4.41] H2O, P < .001). Pressure-control mode was used more frequently in hypoxemic cases but both modes were used equally in hypercapnic cases. Hypoxic respiratory failure (yes/no), odds ratio: 3.9 (95% CI 1.2-12.3, P=.02), Ph (nadir), odds ratio: 0.004 (95% CI 0.000-0.275, P=.01), and base excess, odds ratio: 0.88 (95% CI 0.79-0.98, P=.02) were associated with intensive care mortality.
Although the pressure-control ventilation mode was preferred more frequently in hypoxemic respiratory failure, there was no significant difference between the 2 respiratory modes in terms of length of pediatric intensive care unit stay, MV duration, and mortality. The pressure-regulated volume-control mode seems to be a safer option for physicians who do not have enough experience in using pressurecontrol ventilation mode.
本研究的目的是介绍我们在儿童中使用压力调节容量控制和压力控制通气模式的经验。
对采用压力调节容量控制或压力控制模式进行通气的急性呼吸衰竭患者进行回顾性评估。从儿科重症监护病房数据库收集患者的通气参数(通气的前7天或整个通气期间,如果患者通气时间少于7天)、SpO2、血气和人口统计学数据。
61例患者(中位年龄12 [4.8 - 36.4]个月)纳入研究。40例患者(65.6%)使用压力控制通气模式,21例患者(34.4%)使用压力调节容量控制模式。28例患者(45.9%)患有低氧性呼吸衰竭,44例患者(72.1%)患有高碳酸血症性呼吸衰竭。压力控制通气模式下的呼气末正压中位数(5.4 [4.2 - 6.3] cmH2O)高于压力调节容量控制模式(4.05 [3.68 - 4.41] H2O,P <.001)。压力控制模式在低氧血症病例中使用更频繁,但在高碳酸血症病例中两种模式使用频率相同。低氧性呼吸衰竭(是/否),比值比:3.9(95% CI 1.2 - 12.3,P =.02),最低pH值,比值比:0.004(95% CI 0.000 - 0.275,P =.01),以及碱剩余,比值比:0.88(95% CI 0.79 - 0.98,P =.02)与重症监护病房死亡率相关。
尽管压力控制通气模式在低氧性呼吸衰竭中更常被优先选用,但在儿科重症监护病房住院时间、机械通气持续时间和死亡率方面,这两种呼吸模式之间没有显著差异。对于在使用压力控制通气模式方面经验不足的医生来说,压力调节容量控制模式似乎是一个更安全的选择。