Center for Public Health and Environmental Assessment, United States Environmental Protection Agency, Research Triangle Park, NC.
T.H. Chan School of Public Health, Harvard University, Boston, MA.
Am Heart J. 2022 Jun;248:130-138. doi: 10.1016/j.ahj.2022.02.015. Epub 2022 Mar 7.
Short-term changes in ambient fine particulate matter (PM) increase the risk for unplanned hospital readmissions. However, this association has not been fully evaluated for high-risk patients or examined to determine if the readmission risk differs based on time since discharge. Here we investigate the relation between ambient PM and 30-day readmission risk in heart failure (HF) patients using daily time windows and examine how this risk varies with respect to time following discharge.
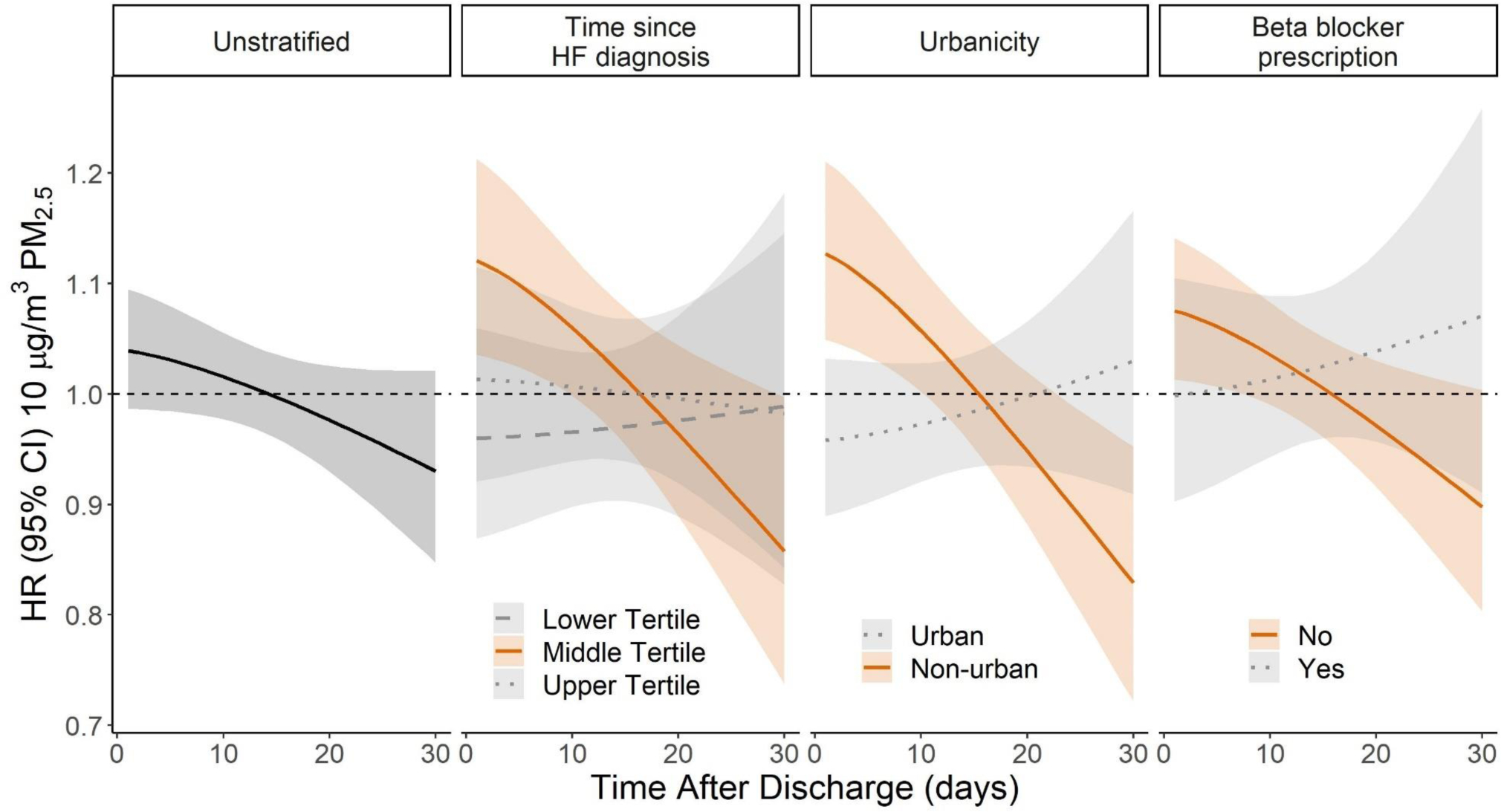
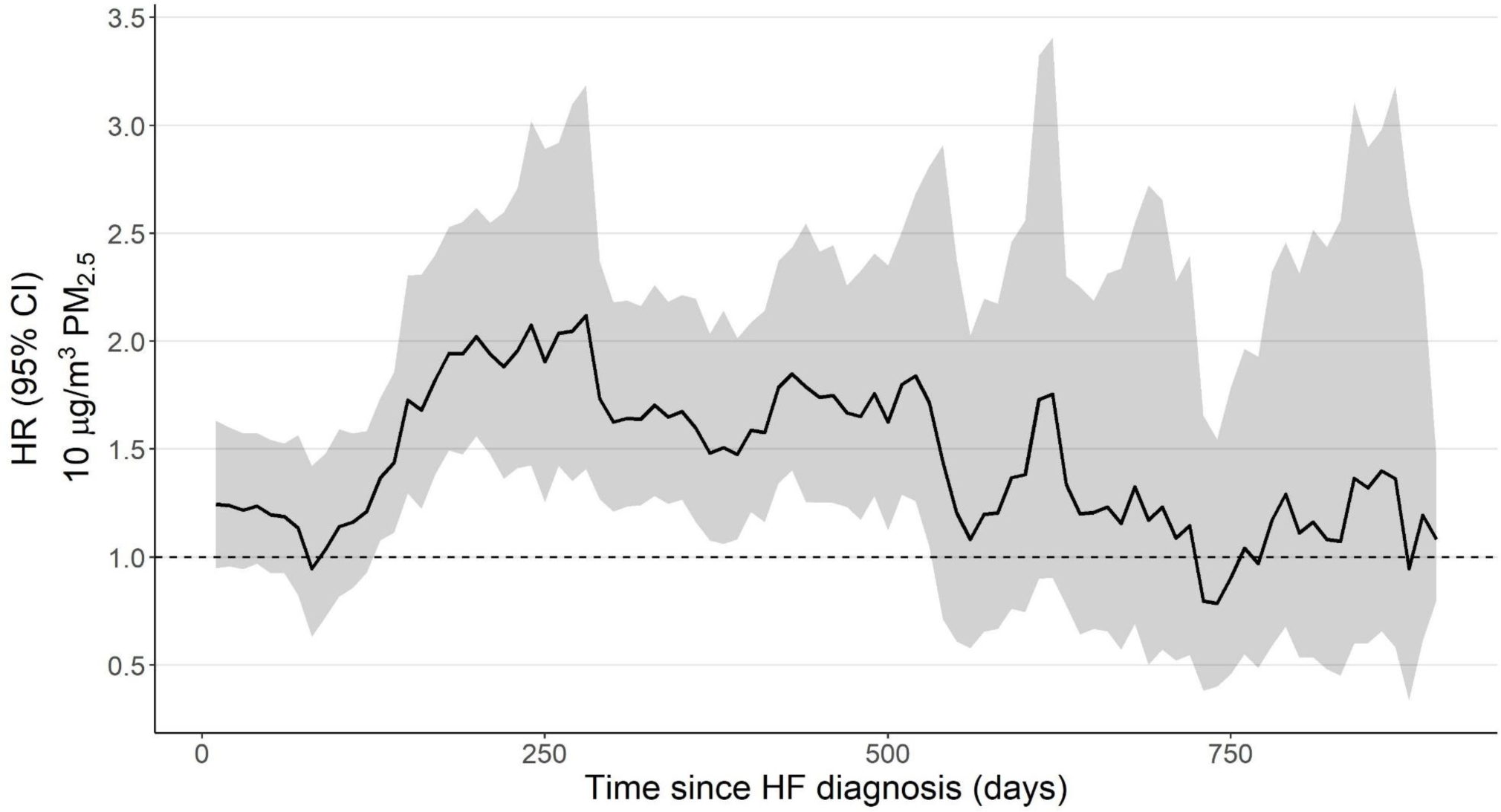
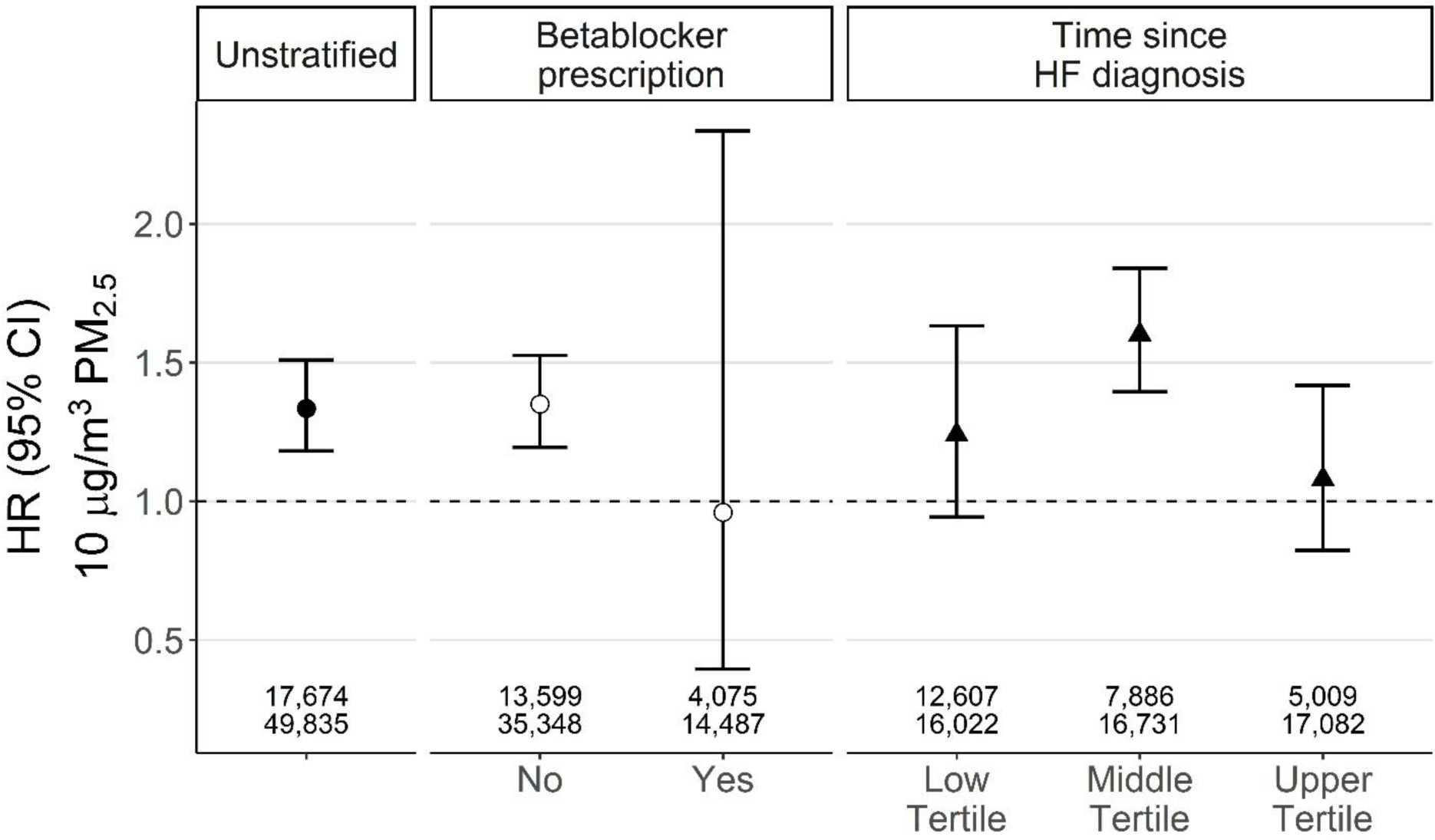
We performed a retrospective cohort study of 17,674 patients with a recorded HF diagnosis between 2004 and 2016. The cohort was identified using the EPA CARES electronic health record resource. The association between ambient daily PM (μg/m) concentration and 30-day readmissions was evaluated using time-dependent Cox proportional hazard models. PM associated readmission risk was examined throughout the 30-day readmission period and for early readmissions (1-3 days post-discharge). Models for 30-day readmissions included a parametric continuous function to estimate the daily PM associated readmission hazard. Fine-resolution ambient PM data were assigned to patient residential address and hazard ratios are expressed per 10 μg/m of PM. Secondary analyses examined potential effect modification based on the time after a HF diagnosis, urbanicity, medication prescription, comorbidities, and type of HF.
The hazard of a PM-related readmission within 3 days of discharge was 1.33 (95% CI 1.18-1.51). This PM readmission hazard was slightly elevated in patients residing in non-urban areas (1.43, 95%CI 1.22-1.67) and for HF patients without a beta-blocker prescription prior to the readmission (1.35; 95% CI 1.19-1.53).
Our findings add to the evidence indicating substantial air quality-related health risks in individuals with underlying cardiovascular disease. Hospital readmissions are key metrics for patients and providers alike. As a potentially modifiable risk factor, air pollution-related interventions may be enacted that might assist in reducing costly and burdensome unplanned readmissions.
短期环境细颗粒物(PM)浓度变化会增加非计划性住院再入院的风险。然而,对于高危患者,尚未充分评估这种相关性,也没有确定再入院风险是否因出院后时间的不同而有所不同。在这里,我们使用每日时间窗研究心力衰竭(HF)患者环境 PM 与 30 天再入院风险之间的关系,并研究这种风险随出院后时间的变化而变化的情况。
我们对 2004 年至 2016 年间有记录的 HF 诊断的 17674 例患者进行了回顾性队列研究。该队列是使用 EPA CARES 电子健康记录资源确定的。使用时间依赖性 Cox 比例风险模型评估环境每日 PM(μg/m)浓度与 30 天再入院之间的关联。在整个 30 天再入院期间以及早期再入院(出院后 1-3 天)期间,检查 PM 相关的再入院风险。30 天再入院模型包括一个参数连续函数,用于估计每日 PM 相关的再入院风险。细颗粒环境 PM 数据被分配给患者的居住地址,风险比表示为每 10 μg/m PM。二次分析检查了基于 HF 诊断后时间、城市性、药物处方、合并症和 HF 类型的潜在效应修饰。
出院后 3 天内与 PM 相关的再入院风险为 1.33(95%CI 1.18-1.51)。在居住在非城市地区的患者中(1.43,95%CI 1.22-1.67)和在再入院前没有β受体阻滞剂处方的 HF 患者中(1.35;95%CI 1.19-1.53),这种 PM 再入院风险略有升高。
我们的研究结果增加了证据,表明空气质量与心血管疾病患者的健康风险有很大关系。医院再入院是患者和提供者共同关注的关键指标。作为一个潜在的可改变的危险因素,可能会实施与空气污染相关的干预措施,以帮助减少昂贵且负担沉重的非计划性再入院。