Ligot Noemie, Elands Sophie, Damien Charlotte, Jodaitis Lise, Sadeghi Meibodi Niloufar, Mine Benjamin, Bonnet Thomas, Guenego Adrien, Lubicz Boris, Naeije Gilles
Department of Neurology, CUB Hôpital Erasme, Université Libre de Bruxelles (ULB), Brussels, Belgium.
Department of Radiology, CUB Hôpital Erasme, Université Libre de Bruxelles (ULB), Brussels, Belgium.
Front Neurol. 2022 Feb 21;13:838192. doi: 10.3389/fneur.2022.838192. eCollection 2022.
Current guidelines suggest that perfusion imaging should only be performed > 6 h after symptom onset. Pathophysiologically, brain perfusion should matter whatever the elapsed time. We aimed to compare relative contribution of recanalization time and stroke core volume in predicting functional outcome in patients treated by endovascular thrombectomy within 6-h of stroke-onset.
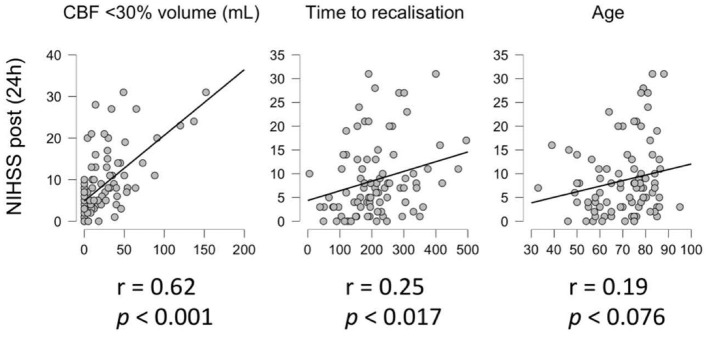
Consecutive patients presenting between January 2015 and June 2021 with (i) an acute ischaemic stroke due to an anterior proximal occlusion, (ii) a successful thrombectomy (TICI >2a) within 6-h of symptom-onset and (iii) CT perfusion imaging were included. Core stroke volume was automatically computed using RAPID software. Two linear regression models were built that included in the null hypothesis the pre-treatment NIHSS score and the hypoperfusion volume (Tmax > 6 s) as confounding variables and 24 h post-recanalization NIHSS and 90 days mRS as outcome variables. Time to recanalization was used as covariate in one model and stroke core volume as covariate in the other.
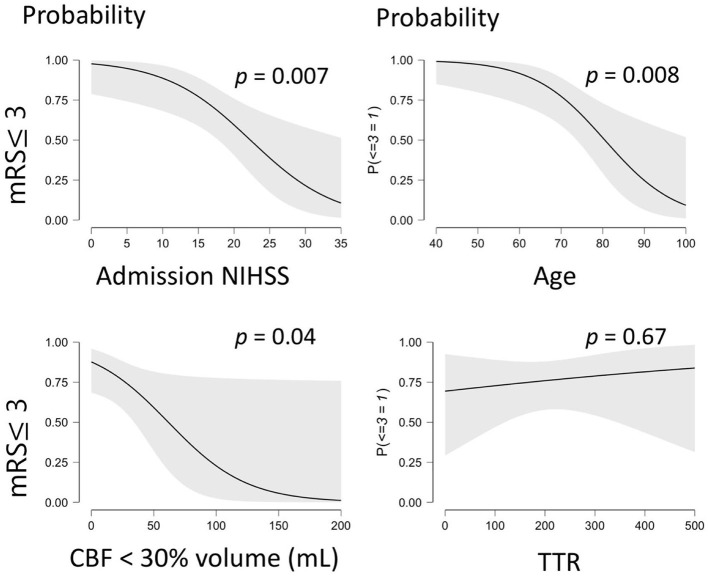
From a total of 377 thrombectomies, 94 matched selection criteria. The Model null hypothesis explained 37% of the variability for 24 h post-recanalization NIHSS and 42% of the variability for 90 days MRS. The core volume as covariate increased outcome variability prediction to 57 and 56%, respectively. Time to recanalization as covariate marginally increased outcome variability prediction from 37 and 34% to 40 and 42.6%, respectively.
Core stroke volume better explains outcome variability in comparison to the time to recanalization in anterior large vessel occlusion stroke with successful thrombectomy done within 6 h of symptoms onset. Still, a large part of outcome variability prediction fails to be explained by the usual predictors.
当前指南建议灌注成像应仅在症状发作后6小时以上进行。从病理生理学角度来看,无论经过多长时间,脑灌注都很重要。我们旨在比较再通时间和卒中核心体积对发病6小时内接受血管内血栓切除术的患者功能结局预测的相对贡献。
纳入2015年1月至2021年6月期间连续就诊的患者,这些患者(i)因前循环近端闭塞导致急性缺血性卒中,(ii)在症状发作6小时内成功进行血栓切除术(脑梗死溶栓分级>2a),(iii)接受了CT灌注成像。使用RAPID软件自动计算核心卒中体积。建立了两个线性回归模型,在原假设中纳入治疗前美国国立卫生研究院卒中量表(NIHSS)评分和低灌注体积(Tmax>6秒)作为混杂变量,再通后24小时NIHSS和90天改良Rankin量表(mRS)作为结局变量。一个模型将再通时间用作协变量,另一个模型将卒中核心体积用作协变量。
在总共377例血栓切除术中,94例符合选择标准。原假设模型分别解释了再通后24小时NIHSS变异性的37%和90天mRS变异性的42%。将核心体积作为协变量可将结局变异性预测分别提高到57%和56%。将再通时间作为协变量可将结局变异性预测从37%和34%分别略微提高到40%和42.6%。
对于症状发作6小时内成功进行血栓切除术的前循环大血管闭塞性卒中,与再通时间相比,核心卒中体积能更好地解释结局变异性。尽管如此,通常的预测指标仍无法解释很大一部分结局变异性预测情况。