Department of Cardiology, Heart and Lung Center, Leiden University Medical Center, Albinusdreef 2, Leiden, 2300 RC, The Netherlands.
Department of Cardiology, Jessa Hospital Hasselt, Hasselt, Belgium.
ESC Heart Fail. 2022 Jun;9(3):1597-1607. doi: 10.1002/ehf2.13857. Epub 2022 Mar 9.
Chronic pressure overload and right ventricular (RV) dysfunction can lead to RV-pulmonary artery (PA) uncoupling in patients with heart failure. The evolution and prognostic values of RV-PA coupling assessed by echocardiography in patients undergoing cardiac resynchronization therapy (CRT) have not been thoroughly investigated. The aim of this study was to evaluate the evolution and prognostic value of tricuspid annular plane systolic excursion (TAPSE)/pulmonary artery systolic pressure (PASP) ratio in CRT recipients.
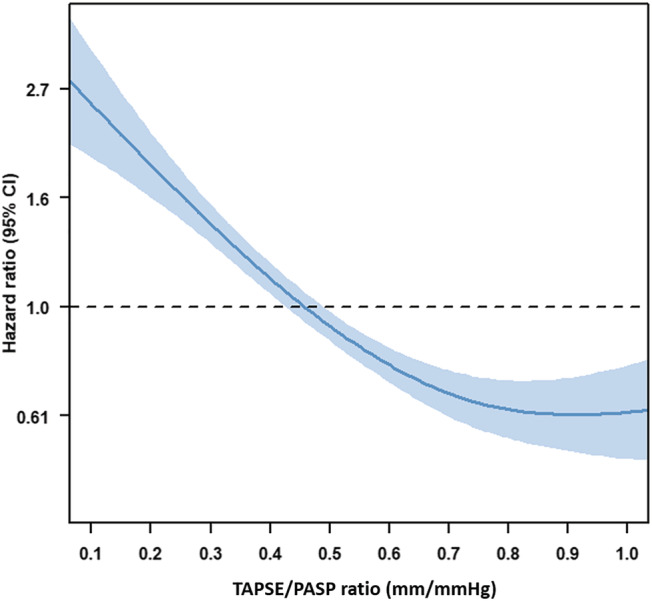
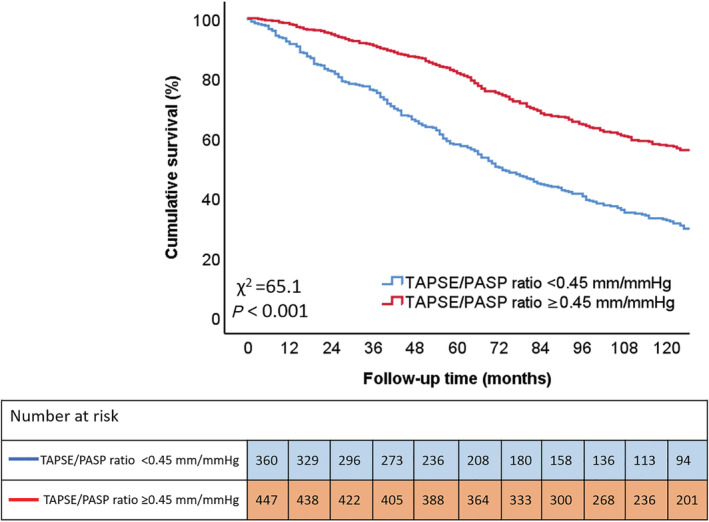
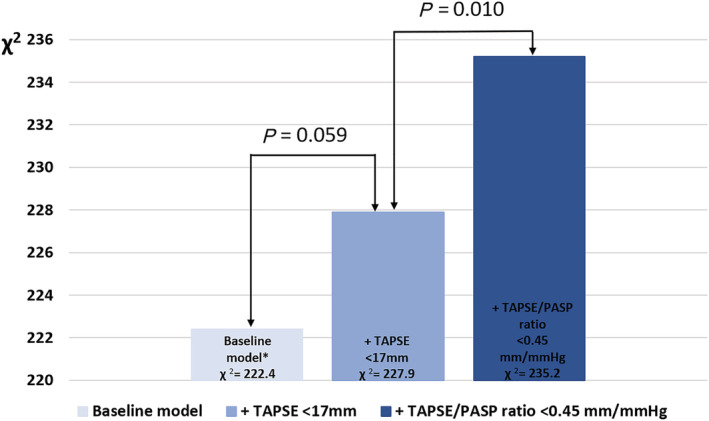
The RV-PA coupling was measured non-invasively with echocardiography using the TAPSE/PASP ratio at baseline and 6 month follow-up in CRT recipients. The cut-off value for TAPSE/PASP uncoupling was derived from spline curve analysis (i.e. <0.45 mm/mmHg). The primary endpoint was all-cause mortality. A total of 807 patients (age 66 ± 11 years, 76% men) were analysed. During a median follow-up of 97 (54-143) months, 483 (60%) patients died. Survival rates at 3 and 5 year follow-up were significantly lower for patients with a TAPSE/PASP ratio <0.45 mm/mmHg (76% and 58%, respectively), compared with those with a TAPSE/PASP ratio ≥0.45 mm/mmHg (91% and 82%, respectively) (P < 0.001). On multivariable analysis, TAPSE/PASP ratio <0.45 mm/mmHg (hazard ratio 1.437; 95% confidence interval: 1.145-1.805; P = 0.002) was independently associated with all-cause mortality, whereas TAPSE <17 mm (hazard ratio 1.237; 95% confidence interval: 0.990-1.546; P = 0.061) was not. In addition, no improvement of the TAPSE/PASP ratio after CRT implantation was independently associated with worse survival.
The TAPSE/PASP ratio at baseline is independently associated with long-term outcomes in CRT recipients. The baseline TAPSE/PASP ratio has incremental value over TAPSE, which does not take account of RV afterload. A lack of improvement in the TAPSE/PASP ratio after CRT implantation is associated with worse survival.
慢性压力超负荷和右心室(RV)功能障碍可导致心力衰竭患者的 RV-肺动脉(PA)解偶联。心脏再同步治疗(CRT)患者中通过超声心动图评估的 RV-PA 偶联的演变和预后价值尚未得到充分研究。本研究旨在评估 CRT 受者三尖瓣环平面收缩期位移(TAPSE)/肺动脉收缩压(PASP)比值的演变和预后价值。
使用 TAPSE/PASP 比值在基线和 CRT 受者 6 个月随访时通过超声心动图无创地测量 RV-PA 偶联。TAPSE/PASP 解偶联的截断值来自样条曲线分析(即<0.45mm/mmHg)。主要终点是全因死亡率。共分析了 807 例患者(年龄 66±11 岁,76%为男性)。在中位数为 97(54-143)个月的随访期间,有 483 例(60%)患者死亡。与 TAPSE/PASP 比值≥0.45mm/mmHg(分别为 76%和 82%)的患者相比,TAPSE/PASP 比值<0.45mm/mmHg 的患者在 3 年和 5 年随访时的生存率明显较低(分别为 58%和 58%)(P<0.001)。多变量分析显示,TAPSE/PASP 比值<0.45mm/mmHg(风险比 1.437;95%置信区间:1.145-1.805;P=0.002)与全因死亡率独立相关,而 TAPSE<17mm(风险比 1.237;95%置信区间:0.990-1.546;P=0.061)则不然。此外,CRT 植入后 TAPSE/PASP 比值无改善与生存率降低独立相关。
基线 TAPSE/PASP 比值与 CRT 受者的长期结局独立相关。基线 TAPSE/PASP 比值与不考虑 RV 后负荷的 TAPSE 相比具有增量价值。CRT 植入后 TAPSE/PASP 比值无改善与生存率降低相关。