Ali Ahmad Hassan, Al Juboori Alhareth, Petroski Gregory F, Diaz-Arias Alberto A, Syed-Abdul Majid M, Wheeler Andrew A, Ganga Rama R, Pitt James B, Spencer Nicole M, Hammoud Ghassan M, Rector R Scott, Parks Elizabeth J, Ibdah Jamal A
Division of Gastroenterology and Hepatology, University of Missouri, Columbia, MO 65211, USA.
Biostatistics and Research Design Unit, School of Medicine, University of Missouri, Columbia, MO 65211, USA.
J Clin Med. 2022 Feb 23;11(5):1201. doi: 10.3390/jcm11051201.
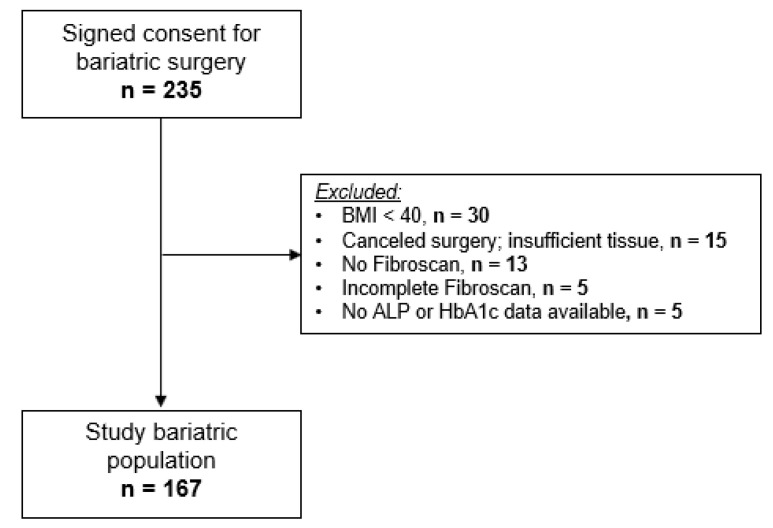
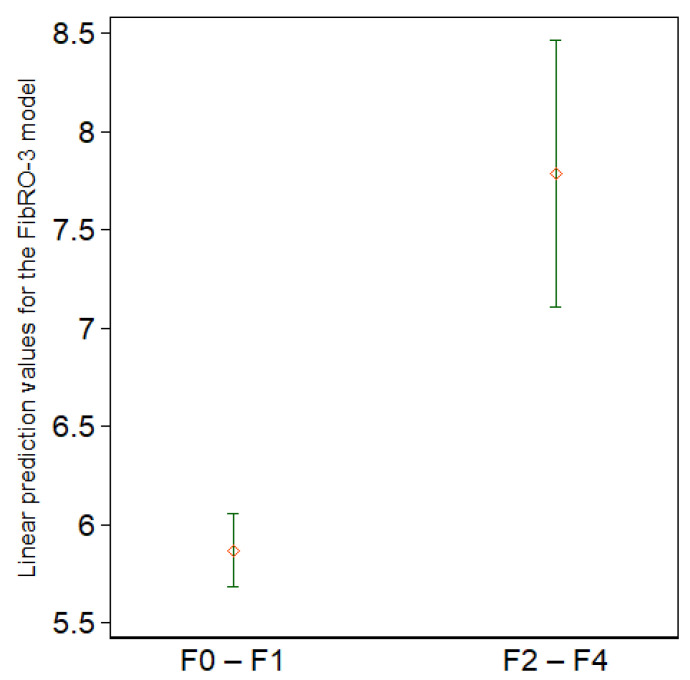
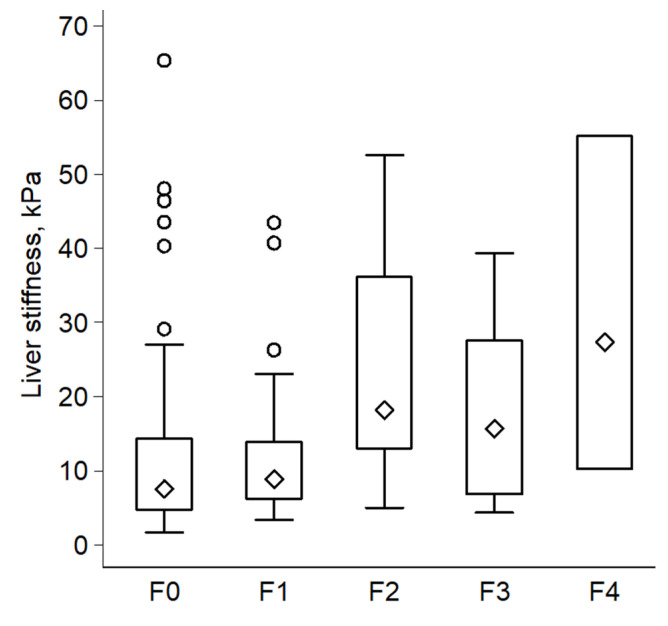
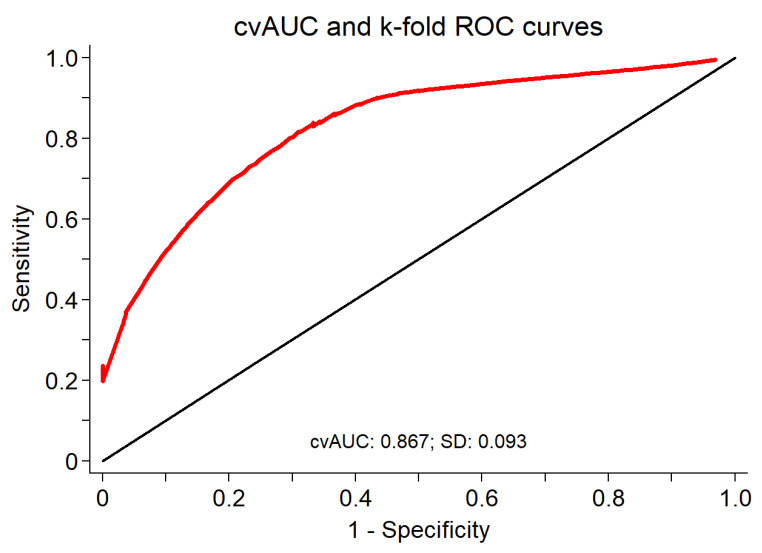
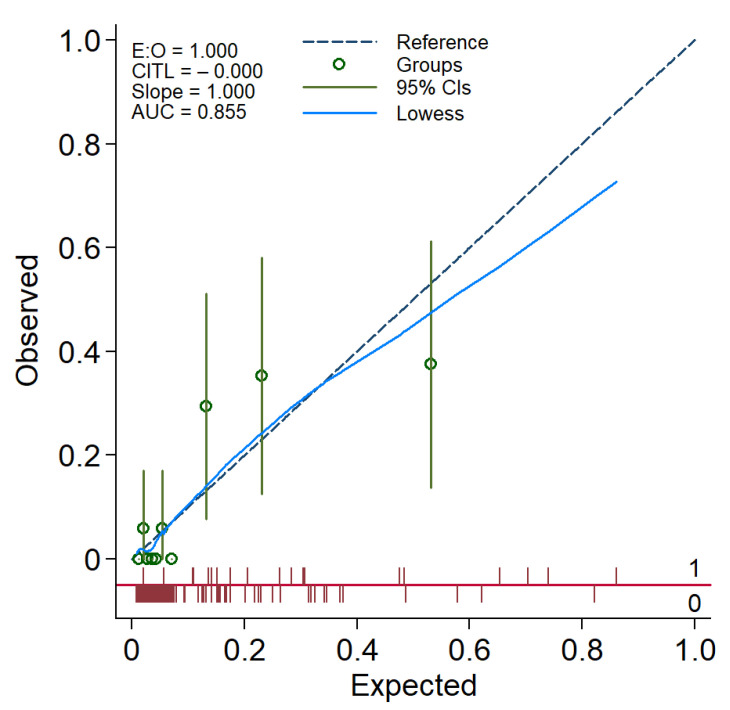
Patients with morbid obesity are at high risk for nonalcoholic fatty liver disease (NAFLD) complicated by liver fibrosis. The clinical utility of transient elastography (TE) by Fibroscan in patients with morbid obesity (body mass index (BMI) ≥ 40 kg/m) is not well-defined. We examined the diagnostic accuracy of Fibroscan in predicting significant liver fibrosis (fibrosis stage ≥2) in morbidly obese patients (BMI ≥ 40 kg/m). Patients scheduled for bariatric surgery were prospectively enrolled. Intraoperative liver biopsy, liver-stiffness measurement (LSM) by Fibroscan (XL probe), and biochemical evaluation were all performed on the same day. The endpoint was significant liver fibrosis defined as fibrosis stage ≥2 based on the Nonalcoholic Steatohepatitis Clinical Research Network. The optimal LSM cutoff value for detecting significant fibrosis was determined by using the Youden Index method. Routine clinical, laboratory, and elastography data were analyzed by stepwise logistic regression analysis to identify predictors of significant liver fibrosis and build a predictive model. An optimal cutoff point of the new model's regression formula for predicting significant fibrosis was determined by using the Youden index method. One hundred sixty-seven patients (mean age, 46.4 years) were included, of whom 83.2% were female. Histological assessment revealed the prevalence of steatohepatitis and significant fibrosis of 40.7% and 11.4%, respectively. The median LSM was found to be significantly higher in the significant fibrosis group compared to those in the no or non-significant fibrosis group (18.2 vs. 7.7 kPa, respectively; = 0.0004). The optimal LSM cutoff for predicting significant fibrosis was 12.8 kPa, with an accuracy of 71.3%, sensitivity of 73.7%, specificity of 70.9%, positive predictive value of 24.6%, negative predictive value of 95.5%, and ROC area of 0.723 (95% CI: 0.62-0.83). Logistic regression analysis identified three independent predictors of significant fibrosis: LSM, hemoglobin A1c, and alkaline phosphatase. A risk score was developed by using these three variables. At an optimal cutoff value of the regression formula, the risk score had an accuracy of 79.6% for predicting significant fibrosis, sensitivity of 89.5%, specificity of 78.4%, positive predictive value of 34.7%, negative predictive value of 98.3%, and ROC area of 0.855 (95% CI: 0.76-0.95). Fibroscan utility in predicting significant liver fibrosis in morbidly obese subjects is limited with accuracy of 71.3%. A model incorporating hemoglobin A1c and alkaline phosphatase with LSM improves accuracy in detecting significant fibrosis in this patient population.
病态肥胖患者发生非酒精性脂肪性肝病(NAFLD)并伴有肝纤维化的风险很高。Fibroscan瞬时弹性成像(TE)在病态肥胖(体重指数(BMI)≥40 kg/m²)患者中的临床应用尚未明确。我们研究了Fibroscan在预测病态肥胖患者(BMI≥40 kg/m²)显著肝纤维化(纤维化分期≥2)方面的诊断准确性。前瞻性纳入计划接受减肥手术的患者。在同一天进行术中肝活检、Fibroscan(XL探头)肝脏硬度测量(LSM)和生化评估。终点为根据非酒精性脂肪性肝炎临床研究网络定义的显著肝纤维化,即纤维化分期≥2。通过约登指数法确定检测显著纤维化的最佳LSM临界值。通过逐步逻辑回归分析对常规临床、实验室和弹性成像数据进行分析,以确定显著肝纤维化的预测因素并建立预测模型。通过约登指数法确定新模型回归公式预测显著纤维化的最佳临界点。纳入167例患者(平均年龄46.4岁),其中83.2%为女性。组织学评估显示脂肪性肝炎和显著纤维化的患病率分别为40.7%和11.4%。发现显著纤维化组的LSM中位数显著高于无或非显著纤维化组(分别为18.2 vs. 7.7 kPa;P = 0.0004)。预测显著纤维化的最佳LSM临界值为12.8 kPa,准确率为71.3%,敏感性为73.7%,特异性为70.9%,阳性预测值为24.6%,阴性预测值为95.5%,ROC曲线下面积为0.723(95%CI:0.62 - 0.83)。逻辑回归分析确定了显著纤维化的三个独立预测因素:LSM、糖化血红蛋白和碱性磷酸酶。利用这三个变量建立了风险评分。在回归公式的最佳临界值时,风险评分预测显著纤维化的准确率为79.6%,敏感性为89.5%,特异性为78.4%,阳性预测值为34.7%,阴性预测值为98.3%,ROC曲线下面积为0.855(95%CI:0.76 - 0.95)。Fibroscan预测病态肥胖受试者显著肝纤维化的效用有限,准确率为71.3%。将糖化血红蛋白、碱性磷酸酶与LSM相结合的模型提高了该患者群体中检测显著纤维化的准确率。