General Medicine and Metabolic Diseases, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Pad. Granelli, Via F Sforza 35, 20122 Milan, Italy.
Department of Pathophysiology and Transplantation, University of Milan, 20122 Milan, Italy.
Int J Mol Sci. 2022 Feb 28;23(5):2707. doi: 10.3390/ijms23052707.
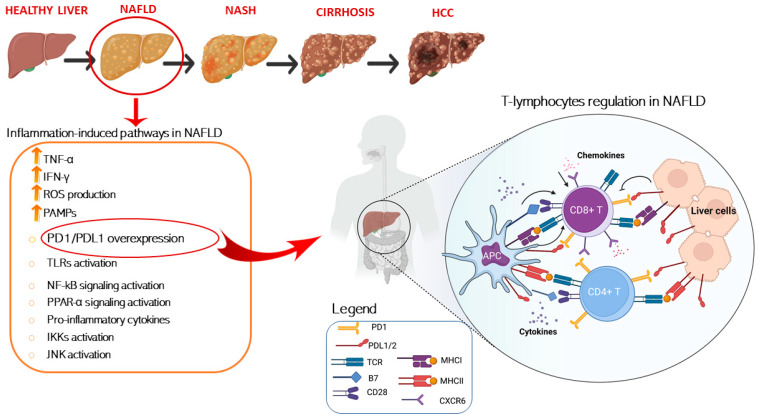
Non-alcoholic fatty liver disease (NAFLD) is characterized by an enhanced activation of the immune system, which predispose the evolution to nonalcoholic steatohepatitis (NASH) and hepatocellular carcinoma (HCC). Resident macrophages and leukocytes exert a key role in the pathogenesis of NAFLD. In particular, CD4+ effector T cells are activated during the early stages of liver inflammation and are followed by the increase of natural killer T cells and of CD8+ T cytotoxic lymphocytes which contribute to auto-aggressive tissue damage. To counteract T cells activation, programmed cell death 1 (PD-1) and its ligand PDL-1 are exposed respectively on lymphocytes and liver cells' surface and can be targeted for therapy by using specific monoclonal antibodies, such as of Nivolumab, Pembrolizumab, and Atezolizumab. Despite the combination of Atezolizumab and Bevacizumab has been approved for the treatment of advanced HCC, PD-1/PD-L1 blockage treatment has not been approved for NAFLD and adjuvant immunotherapy does not seem to improve survival of patients with early-stage HCC. In this regard, different ongoing phase III trials are testing the efficacy of anti-PD-1/PD-L1 antibodies in HCC patients as first line therapy and in combination with other treatments. However, in the context of NAFLD, immune checkpoints inhibitors may not improve HCC prognosis, even worse leading to an increase of CD8+PD-1+ T cells and effector cytokines which aggravate liver damage. Here, we will describe the main pathogenetic mechanisms which characterize the immune system involvement in NAFLD discussing advantages and obstacles of anti PD-1/PDL-1 immunotherapy.
非酒精性脂肪性肝病 (NAFLD) 的特征是免疫系统的增强激活,这使疾病向非酒精性脂肪性肝炎 (NASH) 和肝细胞癌 (HCC) 发展。驻留巨噬细胞和白细胞在 NAFLD 的发病机制中发挥关键作用。特别是,CD4+效应 T 细胞在肝脏炎症的早期阶段被激活,随后自然杀伤 T 细胞和 CD8+T 细胞毒性淋巴细胞增加,导致自身攻击性组织损伤。为了对抗 T 细胞的激活,程序性细胞死亡 1 (PD-1) 和其配体 PDL-1 分别在淋巴细胞和肝细胞表面表达,可以使用特异性单克隆抗体(如 nivolumab、pembrolizumab 和 atezolizumab)来靶向治疗。尽管 Atezolizumab 和 Bevacizumab 的联合已被批准用于治疗晚期 HCC,但 PD-1/PD-L1 阻断治疗尚未被批准用于 NAFLD,辅助免疫疗法似乎也不能改善早期 HCC 患者的生存。在这方面,不同的 III 期临床试验正在测试抗 PD-1/PD-L1 抗体在 HCC 患者中的一线治疗和与其他治疗联合应用的疗效。然而,在 NAFLD 背景下,免疫检查点抑制剂可能不会改善 HCC 的预后,甚至可能导致 CD8+PD-1+T 细胞和效应细胞因子增加,从而加重肝损伤。在这里,我们将描述免疫系统参与 NAFLD 的主要发病机制,讨论抗 PD-1/PDL-1 免疫疗法的优势和障碍。