MRC Integrative Epidemiology Unit, Population Health Sciences, Bristol Medical School, University of Bristol, Bristol, United Kingdom.
Department of Population Health Sciences, Bristol Medical School, University of Bristol, Bristol, United Kingdom.
PLoS One. 2022 Mar 10;17(3):e0265076. doi: 10.1371/journal.pone.0265076. eCollection 2022.
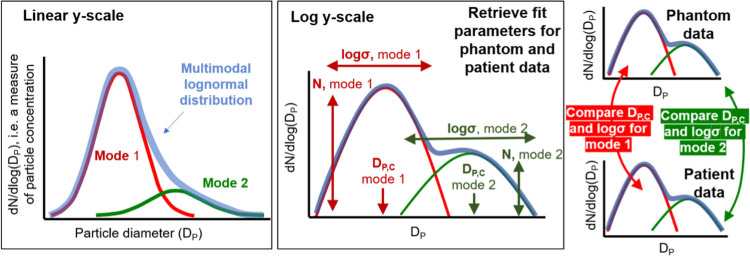
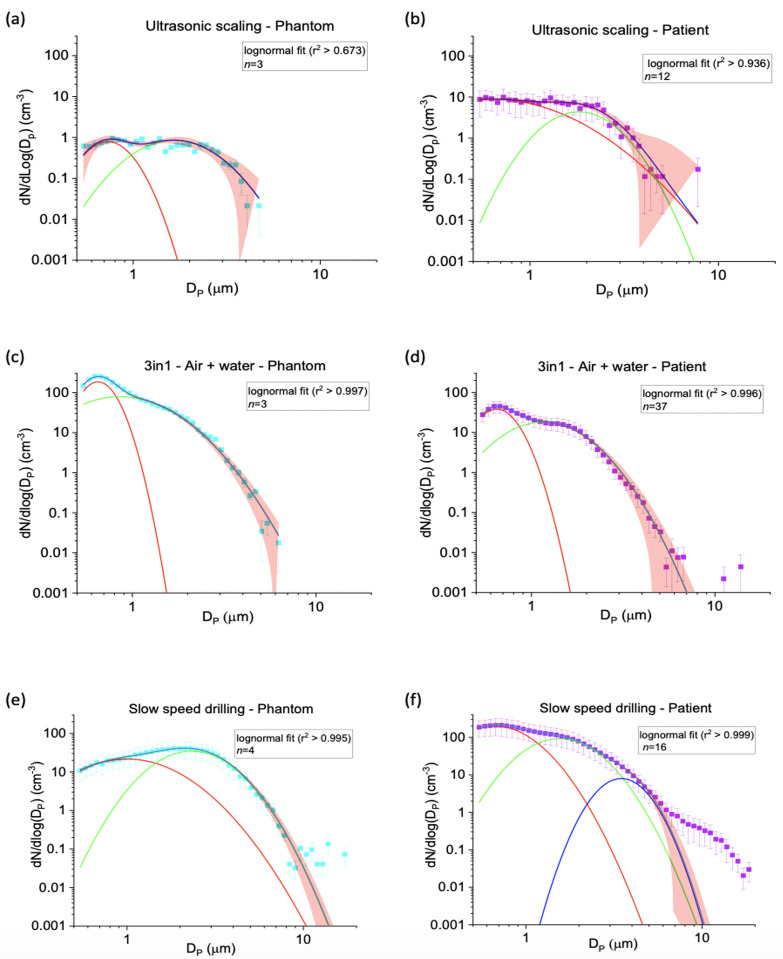
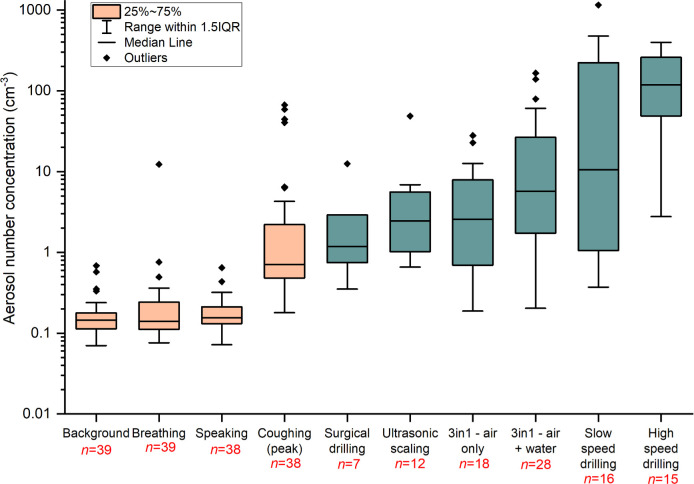
Aerosol generating procedures (AGPs) are defined as any procedure releasing airborne particles <5 μm in size from the respiratory tract. There remains uncertainty about which dental procedures constitute AGPs. We quantified the aerosol number concentration generated during a range of periodontal, oral surgery and orthodontic procedures using an aerodynamic particle sizer, which measures aerosol number concentrations and size distribution across the 0.5-20 μm diameter size range. Measurements were conducted in an environment with a sufficiently low background to detect a patient's cough, enabling confident identification of aerosol. Phantom head control experiments for each procedure were performed under the same conditions as a comparison. Where aerosol was detected during a patient procedure, we assessed whether the size distribution could be explained by the non-salivary contaminated instrument source in the respective phantom head control procedure using a two-sided unpaired t-test (comparing the mode widths (log(σ)) and peak positions (DP,C)). The aerosol size distribution provided a robust fingerprint of aerosol emission from a source. 41 patients underwent fifteen different dental procedures. For nine procedures, no aerosol was detected above background. Where aerosol was detected, the percentage of procedure time that aerosol was observed above background ranged from 12.7% for ultrasonic scaling, to 42.9% for 3-in-1 air + water syringe. For ultrasonic scaling, 3-in-1 syringe use and surgical drilling, the aerosol size distribution matched the non-salivary contaminated instrument source, with no unexplained aerosol. High and slow speed drilling produced aerosol from patient procedures with different size distributions to those measured from the phantom head controls (mode widths log(σ)) and peaks (DP,C, p< 0.002) and, therefore, may pose a greater risk of salivary contamination. This study provides evidence for sources of aerosol generation during common dental procedures, enabling more informed evaluation of risk and appropriate mitigation strategies.
气溶胶产生程序(AGPs)被定义为从呼吸道释放出<5μm 大小的空气传播颗粒的任何程序。哪些牙科程序构成 AGPs 仍存在不确定性。我们使用空气动力学颗粒粒径仪对一系列牙周、口腔手术和正畸程序产生的气溶胶数量浓度进行了量化,该仪器可测量 0.5-20μm 直径范围内的气溶胶数量浓度和粒径分布。在背景足够低以检测到患者咳嗽的环境中进行了测量,从而能够可靠地识别气溶胶。对于每个程序,都在与患者程序相同的条件下进行了 Phantom 头控制实验进行比较。如果在患者程序中检测到气溶胶,则使用双侧非配对 t 检验(比较模式宽度(log(σ))和峰值位置(DP,C))来评估相应 Phantom 头控制程序中未受唾液污染的仪器源是否可以解释气溶胶的粒径分布。气溶胶的粒径分布为来自源的气溶胶排放提供了可靠的指纹。41 名患者接受了十五种不同的牙科程序。在九种程序中,未检测到高于背景的气溶胶。在检测到气溶胶的情况下,气溶胶在高于背景的时间百分比范围从超声洁牙的 12.7%到 3-in-1 空气+水注射器的 42.9%。对于超声洁牙、3-in-1 注射器使用和手术钻孔,气溶胶的粒径分布与受唾液污染的仪器源相匹配,没有未解释的气溶胶。高速和低速钻孔会从患者程序中产生气溶胶,其粒径分布与从 Phantom 头控制中测量的不同(模式宽度 log(σ))和峰值(DP,C,p<0.002),因此可能会带来更大的唾液污染风险。本研究为常见牙科程序中气溶胶产生的来源提供了证据,使我们能够更深入地评估风险并采取适当的缓解策略。