Spicher Barbara, Fischer Kady, Zimmerli Zoe A, Yamaji Kyohei, Ueki Yasushi, Bertschinger Carina N, Jung Bernd, Otsuka Tatsuhiko, Bigler Marius R, Gräni Christoph, von Tengg-Kobligk Hendrik, Räber Lorenz, Eberle Balthasar, Guensch Dominik P
Department of Anaesthesiology and Pain Medicine, Inselspital, University Hospital Bern, University of Bern, Bern, Switzerland.
Department of Cardiology, Inselspital, University Hospital Bern, University of Bern, Bern, Switzerland.
Front Cardiovasc Med. 2022 Feb 24;9:800720. doi: 10.3389/fcvm.2022.800720. eCollection 2022.
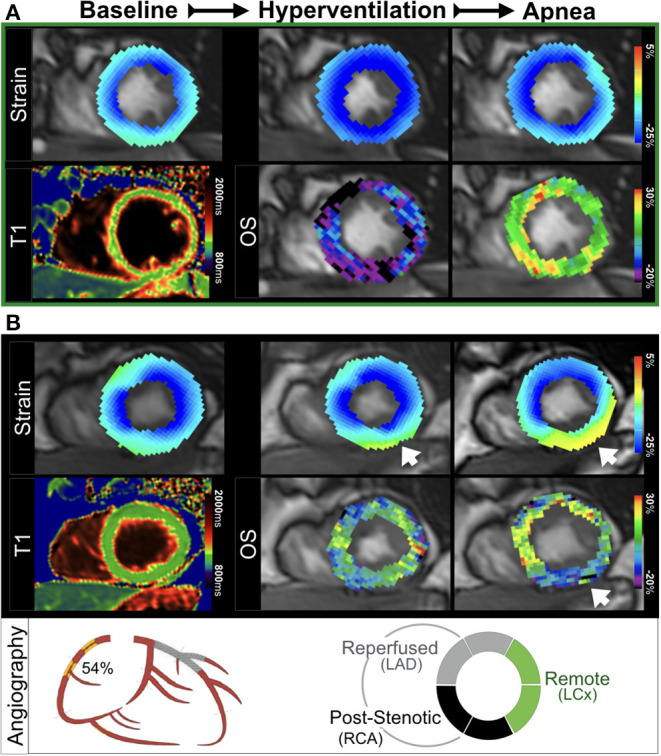
In patients with chronic coronary syndromes, hyperventilation followed by apnea has been shown to unmask myocardium susceptible to inducible deoxygenation. The aim of this study was to assess whether such a provoked response is co-localized with myocardial dysfunction.
A group of twenty-six CAD patients with a defined stenosis (quantitative coronary angiography > 50%) underwent a cardiovascular magnetic resonance (CMR) exam prior to revascularization. Healthy volunteers older than 50 years served as controls ( = 12). Participants hyperventilated for 60s followed by brief apnea. Oxygenation-sensitive images were analyzed for changes in myocardial oxygenation and strain.
In healthy subjects, hyperventilation resulted in global myocardial deoxygenation (-10.2 ± 8.2%, < 0.001) and augmented peak circumferential systolic strain (-3.3 ± 1.6%, < 0.001). At the end of apnea, myocardial signal intensity had increased (+9.1 ± 5.3%, < 0.001) and strain had normalized to baseline. CAD patients had a similar global oxygenation response to hyperventilation (-5.8 ± 9.6%, = 0.085) but showed no change in peak strain from their resting state (-1.3 ± 1.6%), which was significantly attenuated in comparison the strain response observed in controls ( = 0.008). With apnea, the CAD patients showed an attenuated global oxygenation response to apnea compared to controls (+2.7 ± 6.2%, < 0.001). This was accompanied by a significant depression of peak strain (3.0 ± 1.7%, < 0.001), which also differed from the control response ( = 0.025). Regional analysis demonstrated that post-stenotic myocardium was most susceptible to de-oxygenation and systolic strain abnormalities during respiratory maneuvers. CMR measures at rest were unable to discriminate post-stenotic territory ( > 0.05), yet this was significant for both myocardial oxygenation [area under the curve (AUC): 0.88, > 0.001] and peak strain (AUC: 0.73, = 0.023) measured with apnea. A combined analysis of myocardial oxygenation and peak strain resulted in an incrementally higher AUC of 0.91, < 0.001 than strain alone.
In myocardium of patients with chronic coronary syndromes and primarily intermediate coronary stenoses, cine oxygenation-sensitive CMR can identify an impaired vascular and functional response to a vasoactive breathing maneuver stimulus indicative of inducible ischemia.
在慢性冠状动脉综合征患者中,过度通气后呼吸暂停已被证明可揭示易发生诱导性脱氧的心肌。本研究的目的是评估这种诱发反应是否与心肌功能障碍共定位。
一组26例经定量冠状动脉造影显示狭窄程度>50%的冠心病患者在血运重建前接受了心血管磁共振(CMR)检查。50岁以上的健康志愿者作为对照(n = 12)。参与者先过度通气60秒,然后短暂呼吸暂停。分析氧敏感图像以观察心肌氧合和应变的变化。
在健康受试者中,过度通气导致整体心肌脱氧(-10.2±8.2%,P<0.001),并增加了峰值圆周收缩应变(-3.3±1.6%,P<0.001)。呼吸暂停结束时,心肌信号强度增加(+9.1±5.3%,P<0.001),应变恢复到基线水平。冠心病患者对过度通气的整体氧合反应相似(-5.8±9.6%,P = 0.085),但其峰值应变与静息状态相比无变化(-1.3±1.6%),与对照组观察到的应变反应相比显著减弱(P = 0.008)。在呼吸暂停时,与对照组相比,冠心病患者对呼吸暂停的整体氧合反应减弱(+2.7±6.2%,P<0.001)。这伴随着峰值应变的显著降低(3.0±1.7%,P<0.001),这也与对照组的反应不同(P = 0.025)。区域分析表明,狭窄后心肌在呼吸动作期间最易发生脱氧和收缩应变异常。静息时的CMR测量无法区分狭窄后区域(P>0.05),然而,对于呼吸暂停时测量的心肌氧合[曲线下面积(AUC):0.88,P>0.001]和峰值应变(AUC:0.73,P = 0.023)而言这是显著的。心肌氧合和峰值应变的联合分析得出的AUC为0.91,P<0.001,比单独的应变分析更高。
在慢性冠状动脉综合征患者且主要为中度冠状动脉狭窄的心肌中,电影氧敏感CMR可识别对血管活性呼吸动作刺激的血管和功能反应受损,这表明存在诱导性缺血。