Neuroradiology Unit, Department of Experimental and Clinical Biomedical Sciences "Mario Serio", University of Florence, Florence.
Neuroradiology Unit, Department of Radiology, Careggi University Hospital, Florence, Italy.
Ann Neurol. 2022 Jun;91(6):878-888. doi: 10.1002/ana.26354. Epub 2022 Apr 2.
The objective of this paper was to explore the utility of time to maximum concentration (T )-based target mismatch on computed tomography perfusion (CTP) in predicting radiological and clinical outcomes in patients with acute ischemic stroke (AIS) with anterior circulation large vessel occlusion (LVO) selected for endovascular treatment (EVT).
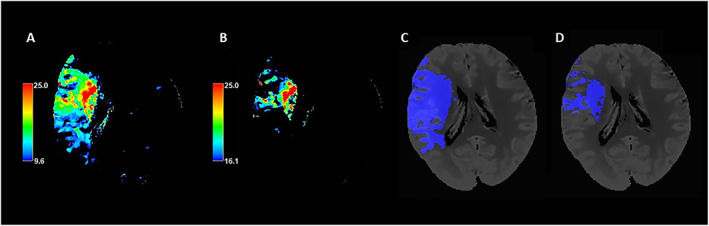
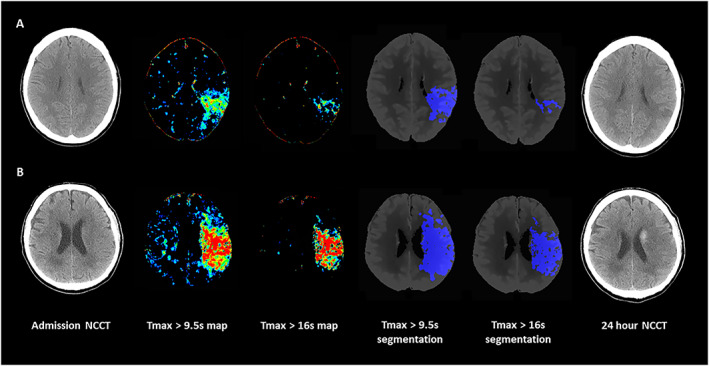
Patients with AIS underwent CTP within 24 hours from onset followed by EVT. Critically hypoperfused tissue and ischemic core volumes were automatically calculated using T thresholds >9.5 seconds and >16 seconds, respectively. The difference between T > 9.5 seconds and T > 16 seconds volumes and the ratio between T > 9.5 seconds and T > 16 seconds volumes were considered ischemic penumbra and T mismatch ratio, respectively. Final infarct volume (FIV) was measured on follow-up non-contrast computed tomography (CT) at 24 hours. Favorable clinical outcome was defined as 90-day modified Rankin Scale 0 to 2. Predictors of FIV and outcome were assessed with multivariable logistic regression. Optimal T volumes for identification of good outcome was defined using receiver operating curves.
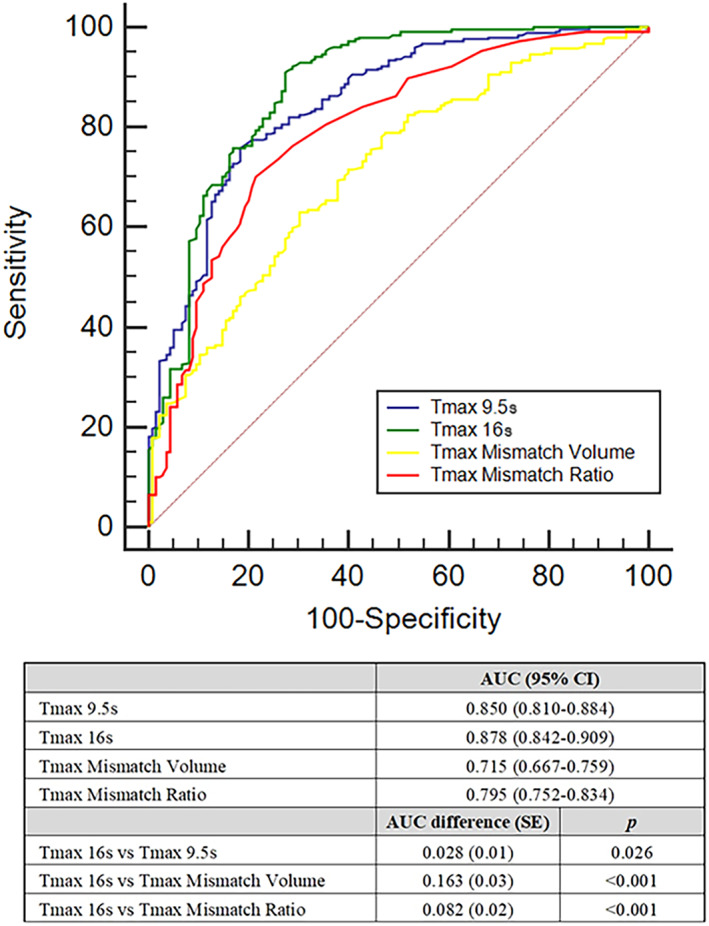
A total of 393 patients were included, of whom 298 (75.8%) achieved successful recanalization and 258 (65.5%) achieved good outcome. In multivariable analyses, all T parameters were independent predictors of FIV and outcome. T > 16 seconds volume had the strongest association with FIV (beta coefficient = 0.596 p <0.001) and good outcome (odds ratio [OR] = 0.96 per 1 ml increase, 95% confidence interval [CI] = 0.95-0.97, p < 0.001). T > 16 seconds volume had the highest discriminative ability for good outcome (area under the curve [AUC] = 0.88, 95% CI = 0.842-0.909). A T > 16 seconds volume of ≤67 ml best identified subjects with favorable outcome (sensitivity = 0.91 and specificity = 0.73).
T target mismatch predicts radiological and clinical outcomes in patients with AIS with LVO receiving EVT within 24 hours from onset. ANN NEUROL 2022;91:878-888.
本文旨在探讨基于时间至最大浓度(T)的目标不匹配在计算机断层灌注(CTP)中的应用价值,以预测接受血管内治疗(EVT)的前循环大血管闭塞(LVO)急性缺血性脑卒中(AIS)患者的影像学和临床结局。
发病后 24 小时内行 CTP 检查,对 AIS 患者进行 EVT。使用 T 阈值>9.5 秒和>16 秒自动计算严重低灌注组织和缺血核心体积。T>9.5 秒与 T>16 秒体积之间的差异和 T>9.5 秒与 T>16 秒体积之间的比值分别被认为是缺血半暗带和 T 不匹配比。在 24 小时的随访非对比 CT 上测量最终梗死体积(FIV)。90 天改良 Rankin 量表 0 至 2 分定义为良好临床结局。采用多变量逻辑回归评估 FIV 和结局的预测因子。使用受试者工作特征曲线确定最佳 T 体积以识别良好结局。
共纳入 393 例患者,其中 298 例(75.8%)成功再通,258 例(65.5%)获得良好结局。多变量分析中,所有 T 参数均为 FIV 和结局的独立预测因子。T>16 秒体积与 FIV 相关性最强(β系数=0.596,p<0.001)和良好结局(优势比[OR]每增加 1 ml 为 0.96,95%置信区间[CI]为 0.95-0.97,p<0.001)。T>16 秒体积对良好结局的区分能力最高(曲线下面积[AUC]为 0.88,95%CI 为 0.842-0.909)。T>16 秒体积≤67ml 时,最佳识别出预后良好的患者(灵敏度为 0.91,特异性为 0.73)。
T 目标不匹配可预测发病后 24 小时内接受 EVT 的前循环 LVO-AIS 患者的影像学和临床结局。