Department of Rheumatology & Clinical Immunology, University Medical Center Utrecht, Utrecht.
Department of Dermatology, LangeLand Ziekenhuis, Zoetermeer.
Rheumatology (Oxford). 2022 Nov 2;61(11):4232-4244. doi: 10.1093/rheumatology/keac129.
The use of systemic glucocorticoids (SGCs) is traditionally discouraged in the treatment of PsA and psoriasis due to the risk of psoriatic flares. However, despite this recommendation, SGCs are frequently prescribed for these patients. In this study we reappraise the old paradigm that SGCs are contra-indicated in the treatment of PsA and psoriasis.
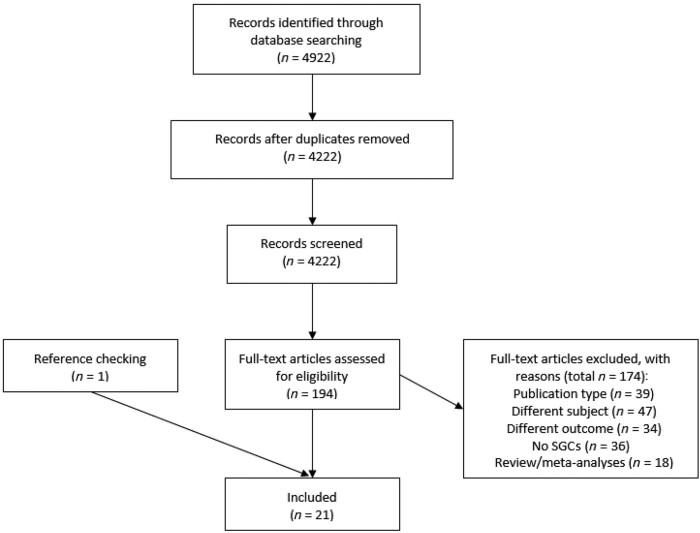
A systematic search of MEDLINE, EMBASE and the Cochrane Library databases was performed in November 2019 to identify articles on any SGC use compared with no use in the PsA and psoriasis population. Topical glucocorticoid treatment was excluded. Our two primary outcomes focused on the prescribing characteristics and the occurrence of any type of flare.
Our search yielded 4922 articles, and of these 21 full-text articles were eligible for inclusion. There were 11 retro- and prospective cohorts involving a total of 4,171,307 patients. Of these, 6727 (37.82%) of the patients with PsA and 1 460 793 (35.17%) of the patients with psoriasis were treated with any type of SGC. Ten observational/interventional studies did not report an increased risk or occurrence of psoriatic flares related to SGC use.
Our results indicate that SGCs are frequently prescribed for PsA and psoriasis patients. The occurrence of psoriatic flares appears to be low upon SGC exposure. In patients with a clear indication for SGCs, e.g. in need of rapid anti-inflammatory therapy or bridging of therapies, the use of SGCs should be considered in view of the low risk of skin flaring. It remains of importance to weigh risks for short- and long-term SGC-related side effects in clinical decision making.
由于发生银屑病样发作的风险,传统上不建议在治疗银屑病关节炎(PsA)和银屑病时使用全身性糖皮质激素(SGCs)。然而,尽管有这一建议,SGCs 仍经常被开给这些患者。在这项研究中,我们重新评估了 SGCs 治疗 PsA 和银屑病禁忌的旧观点。
我们于 2019 年 11 月对 MEDLINE、EMBASE 和 Cochrane 图书馆数据库进行了系统检索,以确定任何 SGC 使用与 PsA 和银屑病人群中不使用 SGC 的比较的文章。排除局部糖皮质激素治疗。我们的两个主要结局集中在处方特征和任何类型发作的发生上。
我们的搜索结果产生了 4922 篇文章,其中 21 篇全文文章符合纳入标准。有 11 项回顾性和前瞻性队列研究,共涉及 4171307 名患者。其中,6727 名(37.82%)PsA 患者和 1460793 名(35.17%)银屑病患者接受了任何类型的 SGC 治疗。有 10 项观察性/干预性研究没有报告与 SGC 使用相关的银屑病发作风险或发生率增加。
我们的结果表明,SGCs 经常被开给 PsA 和银屑病患者。在 SGC 暴露后,银屑病发作的发生率似乎较低。对于有明确 SGC 适应证的患者,例如需要快速抗炎治疗或治疗桥接,应考虑使用 SGC,因为皮肤发作的风险较低。在临床决策中权衡 SGC 相关短期和长期副作用的风险仍然很重要。