Lee Chun-Yuan, Lin Yi-Pei, Wang Sheng-Fan, Lu Po-Liang
Division of Infectious Diseases, Department of Internal Medicine, Kaohsiung Medical University Hospital, No. 100, Ziyou 1st Rd., Sanmin Dist., Kaohsiung City, Taiwan ROC.
Graduate Institute of Medicine, College of Medicine, Kaohsiung Medical University, No. 100, Ziyou 1st Rd., Sanmin Dist., Kaohsiung City, Taiwan ROC.
Infect Dis Ther. 2022 Jun;11(3):1033-1056. doi: 10.1007/s40121-022-00619-7. Epub 2022 Mar 18.
Late initiation (LI) of combination antiretroviral therapy (cART)-defined as having a CD4 count of < 200 cells/μL or an AIDS-defining disease at cART initiation-has detrimental outcomes but remains prevalent worldwide, with LI trends and etiologies following the implementation of various HIV policies remaining underinvestigated. We assessed key concerns, characterized the determinants of various statuses at cART initiation, and evaluated the effects of those statuses on all-cause mortality after cART initiation.
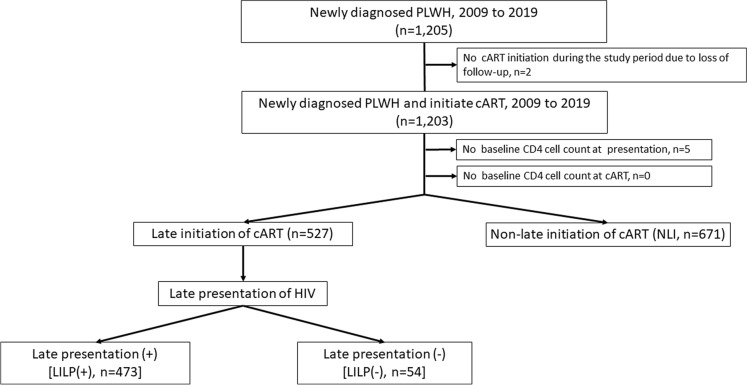
This multicenter retrospective cohort study enrolled 1198 patients with newly diagnosed HIV infection during 2009-2019 who were grouped by status at cART initiation: those without LI (non-LI group, 56.01%); those with LI but without late presentation (LP) of HIV (LP: a CD4 + count of < 200 cells/μL at HIV presentation or AIDS events ≤ 3 months of HIV diagnosis) [LILP(-) group, 4.51%]; and those with LI and with LP of HIV [LILP(+) group, 39.48%]. Joinpoint regression was used to identify changes in LI proportion.
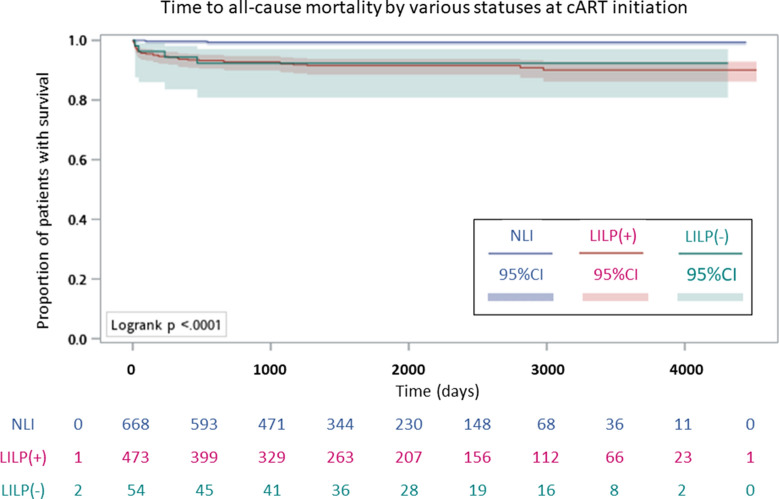
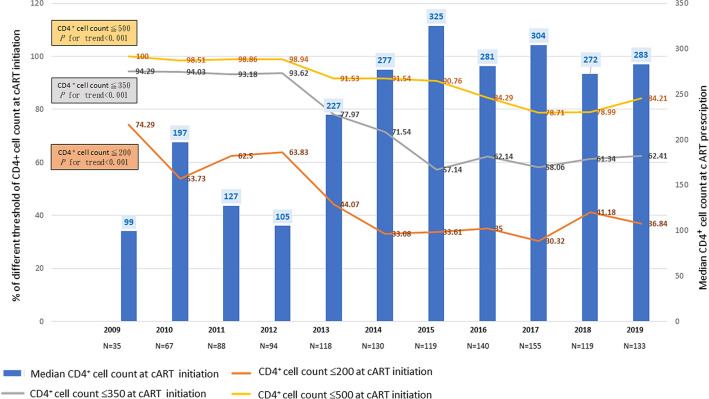
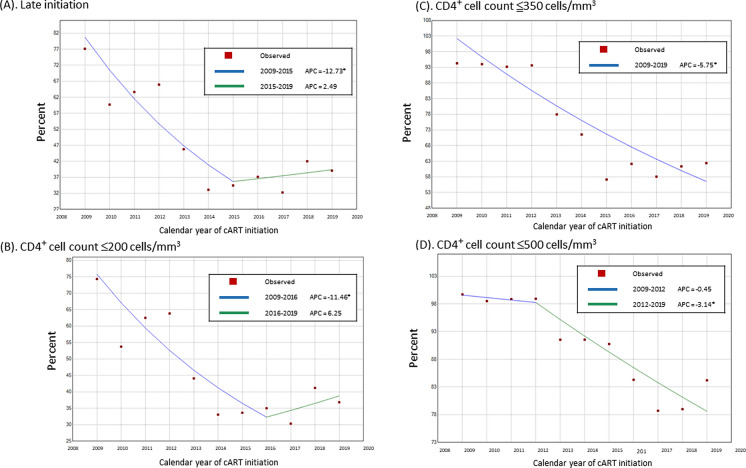
The median CD4 count at cART initiation increased significantly between 2009 (98 cells/μL) and 2015 (325 cells/μL) and stabilized thereafter (P for trend < 0.001). For LI, we identified one joinpoint in 2015: a substantial decrease from 77.14% in 2009 to 34.45% in 2015, followed by a nonsignificant increase to 39.1% in 2019. Overall, LILP(+) explained 89.8% of LI, without significant changes (92.59% in 2009 to 94.23% in 2019). In addition to HIV diagnosis during 2009-2012, multinomial logistic regression identified an age over 30 years and acute HIV infection as risk factors for LILP(+) and LILP(-), respectively. LILP(-) and LILP(+) were associated with a higher all-cause mortality risk.
Given the rise in LI from 2015 in the era of treat-all and rapid cART initiation, strategic interventions to increase earlier cART initiation must be intensified in Taiwan, especially among populations with delayed access to HIV testing services.
联合抗逆转录病毒疗法(cART)启动延迟(LI)定义为在开始cART时CD4细胞计数<200个/μL或患有艾滋病定义疾病,其会产生不良后果,但在全球范围内仍然普遍存在,在实施各种HIV政策后,LI的趋势和病因仍未得到充分研究。我们评估了关键问题,确定了cART启动时各种状态的决定因素,并评估了这些状态对cART启动后全因死亡率的影响。
这项多中心回顾性队列研究纳入了2009年至2019年期间新诊断为HIV感染的1198例患者,根据cART启动时的状态进行分组:无LI者(非LI组,56.01%);有LI但无HIV晚期表现(LP:HIV表现时CD4+细胞计数<200个/μL或艾滋病事件发生在HIV诊断后≤3个月)者[LILP(-)组,4.51%];以及有LI且有HIV晚期表现者[LILP(+)组,39.48%]。采用Joinpoint回归分析确定LI比例的变化。
2009年(98个/μL)至2015年(325个/μL)期间,cART启动时的CD4细胞计数中位数显著增加,此后趋于稳定(趋势P<0.001)。对于LI,我们在2015年确定了一个Joinpoint:从2009年的77.14%大幅下降至2015年的34.45%,随后在2019年无显著增加至39.1%。总体而言,LILP(+)占LI的89.8%,无显著变化(2009年为92.59%,2019年为94.23%)。除了2009年至2012年期间的HIV诊断外,多项逻辑回归分析确定年龄超过30岁和急性HIV感染分别是LILP(+)和LILP(-)的危险因素。LILP(-)和LILP(+)与全因死亡风险较高相关。
鉴于在普遍治疗和快速启动cART时代,LI自2015年以来有所上升,台湾地区必须加强战略干预措施,以更早地启动cART,特别是在获得HIV检测服务延迟的人群中。