Lifespan and Population Health Unit, School of Medicine, University of Nottingham, Nottingham, UK.
WHO Collaborating Centre for Mental Health Research & Capacity Building, Department of Psychiatry, School of Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia.
Lancet Glob Health. 2022 Apr;10(4):e530-e542. doi: 10.1016/S2214-109X(22)00027-4.
Community-based rehabilitation (CBR) is recommended to address the social and clinical needs of people with schizophrenia in resource-poor settings. We evaluated the effectiveness of CBR at reducing disability at 12 months in people with schizophrenia who had disabling illness after having had the opportunity to access facility-based care for 6 months METHODS: This cluster-randomised controlled trial was conducted in a rural district of Ethiopia. Eligible clusters were subdistricts in Sodo district that had not participated in the pilot study. Available subdistricts were randomised (in a 1:1 ratio) to either the intervention group (CBR plus facility-based care) or to the control group (facility-based care alone). An optimisation procedure (accounting for the subdistrict mean WHO Disability Assessment Schedule (WHODAS) score and the potential number of participants per subdistrict) was applied for each of the eight health facilities in the district. An independent statistician, masked to the intervention or control label, used a computer programme to randomly choose the allocation sequence from the set of optimal ones. We recruited adults with disabling illness as a result of schizophrenia. The subdistricts were eligible for inclusion if they included participants that met the eligibility criteria. Researchers recruiting and assessing participants were masked to allocation status. Facility-based care was a task-shared model of mental health care integrated within primary care. CBR was delivered by lay workers over a 12-month period, comprising of home visits (psychoeducation, adherence support, family intervention, and crisis management) and community mobilisation. The primary outcome was disability, measured with the proxy-rated 36-item WHODAS score at 12 months. The subdistricts that had primary outcome data available were included in the primary analysis. This study is registered with ClinicalTrials.gov, NCT02160249.
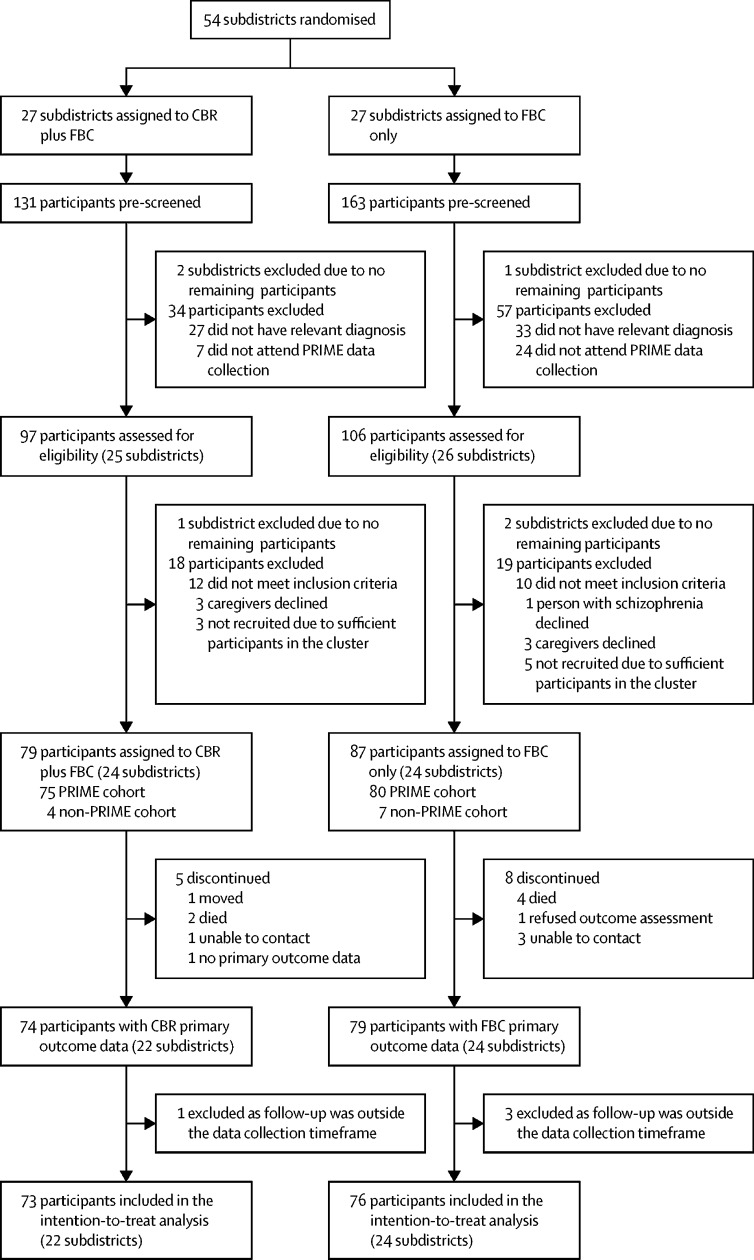
Enrolment took place between Sept 16, 2015 and Mar 11, 2016. 54 subdistricts were randomised (27 to the CBR plus facility-based care group and 27 to the facility-based care group). After exclusion of subdistricts without eligible participants, we enrolled 79 participants (66% men and 34% women) from 24 subdistricts assigned to CBR plus facility-based care and 87 participants (59% men and 41% women) from 24 subdistricts assigned to facility-based care only. The primary analysis included 149 (90%) participants in 46 subdistricts (73 participants in 22 subdistricts in the CBR plus facility-based care group and 76 participants in 24 subdistricts in the facility-based care group). At 12 months, the mean WHODAS scores were 46·1 (SD 23·3) in the facility-based care group and 40·6 (22·5) in the CBR plus facility-based care group, indicating a favourable intervention effect (adjusted mean difference -8·13 [95% CI -15·85 to -0·40]; p=0·039; effect size 0·35). Four (5%) CBR plus facility-based care group participants and nine (10%) facility-based care group participants had one or more serious adverse events (death, suicide attempt, and hospitalisation).
CBR delivered by lay workers combined with task-shared facility-based care, was effective in reducing disability among people with schizophrenia. The RISE study CBR model is particularly relevant to low-income countries with few mental health specialists.
Wellcome Trust.
社区康复(CBR)被推荐用于解决资源匮乏环境中精神分裂症患者的社会和临床需求。我们评估了 CBR 在使患者有机会接受机构护理 6 个月后,在 12 个月时减少精神分裂症患者残疾的效果。
这是一项在埃塞俄比亚农村地区进行的集群随机对照试验。符合条件的集群为索多区没有参与试点研究的分区。现有的分区以 1:1 的比例随机分配到干预组(CBR 加机构护理)或对照组(仅机构护理)。针对每个区的 8 个卫生机构,采用了一种优化程序(考虑了分区平均的世界卫生组织残疾评估量表(WHODAS)评分和每个分区潜在的参与者人数)。独立的统计学家对干预或对照标签进行了屏蔽,使用计算机程序从最佳的一组中随机选择分配顺序。我们招募了因精神分裂症而导致残疾的成年人。如果分区包含符合资格标准的参与者,则有资格参加。招募和评估参与者的研究人员对分配情况进行了屏蔽。机构护理是一种基于任务分担的心理健康护理模式,整合在初级保健中。CBR 由非专业人员在 12 个月的时间内提供,包括家访(心理教育、遵医行为支持、家庭干预和危机管理)和社区动员。主要结局是残疾,采用 36 项代理评定的 WHODAS 评分在 12 个月时进行测量。有主要结局数据的分区被纳入主要分析。本研究在 ClinicalTrials.gov 注册,编号为 NCT02160249。
招募工作于 2015 年 9 月 16 日至 2016 年 3 月 11 日进行。随机分配了 54 个分区(27 个分配给 CBR 加机构护理组,27 个分配给机构护理组)。在排除没有合格参与者的分区后,我们从 24 个分配给 CBR 加机构护理的分区中招募了 79 名参与者(66%为男性,34%为女性),从 24 个分配给机构护理的分区中招募了 87 名参与者(59%为男性,41%为女性)。主要分析包括来自 46 个分区的 149 名(90%)参与者(73 名参与者来自 22 个分区的 CBR 加机构护理组,76 名参与者来自 24 个分区的机构护理组)。在 12 个月时,机构护理组的 WHODAS 评分平均为 46.1(23.3),CBR 加机构护理组的评分平均为 40.6(22.5),表明干预效果良好(调整后的平均差异-8.13 [95%CI-15.85 至-0.40];p=0.039;效应量 0.35)。CBR 加机构护理组有 4 名(5%)参与者和机构护理组有 9 名(10%)参与者发生了一个或多个严重不良事件(死亡、自杀企图和住院)。
由非专业人员提供的 CBR 与基于任务分担的机构护理相结合,在减少精神分裂症患者的残疾方面是有效的。RISE 研究的 CBR 模式特别适用于精神卫生专家较少的低收入国家。
惠康信托基金会。