Cucchetti Alessandro, Aldrighetti Luca, Ratti Francesca, Ferrero Alessandro, Guglielmi Alfredo, Giuliante Felice, Cillo Umberto, Mazzaferro Vincenzo, De Carlis Luciano, Ercolani Giorgio
Department of Medical and Surgical sciences - DIMEC; Alma Mater Studiorum, University of Bologna, Bologna, Italy.
Morgagni, Pierantoni Hospital, Forlì, Italy.
J Hepatobiliary Pancreat Sci. 2022 May;29(5):521-530. doi: 10.1002/jhbp.1141. Epub 2022 Apr 5.
BACKGROUND/PURPOSE: Quality measures in surgery are important to establish appropriate levels of care and to develop improvement strategies. The purpose of this study was to provide risk-adjusted outcome measures after laparoscopic liver resection (LLR).
Data from a prospective, multicenter database involving 4318 patients submitted to LLRs in 41 hospitals from an intention-to-treat approach (2014-2020) were used to analyze heterogeneity (I ) among centers and to develop a risk-adjustment model on outcome measures through multivariable mixed-effect models to account for confounding due to case-mix.
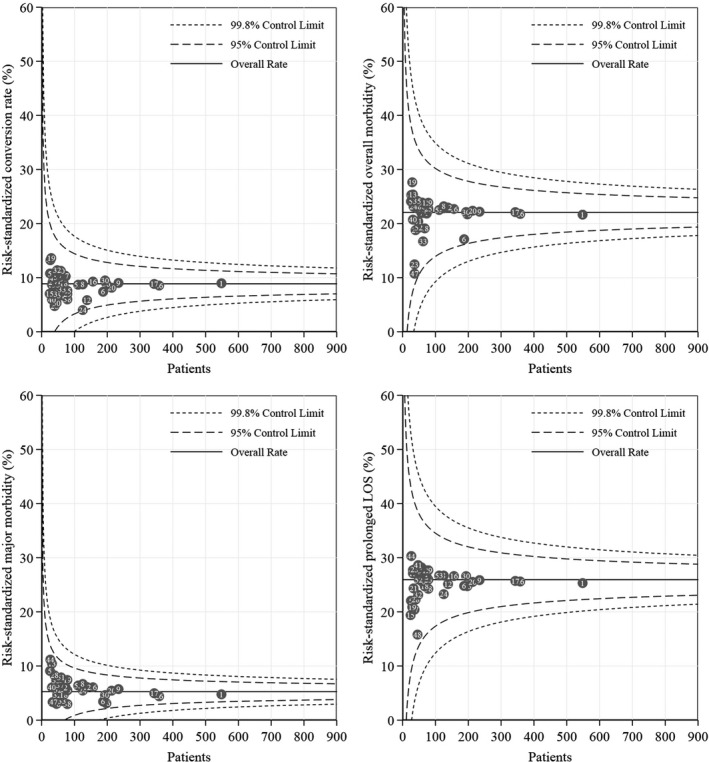
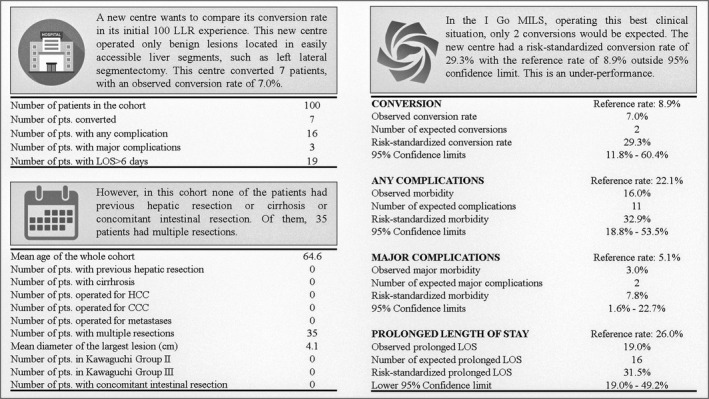
Involved hospitals operated on very different patients: the largest heterogeneity was observed for operating in the presence of previous abdominal surgery (I :79.1%), in cirrhotic patients (I :89.3%) suffering from hepatocellular carcinoma (I :88.6%) or requiring associated intestinal resections (I :82.8%) and in regard to technical complexity (I for the most complex LLRs: 84.1%). These aspects determined substantial or large heterogeneity in overall morbidity (I :84.9%), in prolonged in-hospital stay (I :86.9%) and in conversion rate (I :73.4%). Major complication had medium heterogeneity (I :46.5%). The heterogeneity of mortality was null. Risk-adjustment accounted for all of this variability and the final risk-standardized conversion rate was 8.9%, overall morbidity was 22.1%, major morbidity was 5.1% and prolonged in-hospital stay was 26.0%. There were no outliers among the 41 participating centers. An online tool was provided.
A benchmark for LLRs including all eligible patients was provided, suggesting that surgeons can act accordingly in the interest of the patient, modifying their approach in relation to different indications and different experience, but finally providing the same quality of care.
背景/目的:手术中的质量指标对于确立适当的医疗水平以及制定改进策略至关重要。本研究的目的是提供腹腔镜肝切除(LLR)术后的风险调整后结局指标。
采用来自前瞻性多中心数据库的数据,该数据库纳入了2014 - 2020年期间41家医院4318例接受LLR手术的患者,采用意向性分析方法,以分析各中心之间的异质性(I²),并通过多变量混合效应模型建立结局指标的风险调整模型,以考虑病例组合导致的混杂因素。
参与研究的医院所治疗的患者差异很大:在既往有腹部手术史的患者中进行手术时观察到最大的异质性(I²:79.1%),在患有肝细胞癌(I²:88.6%)或需要联合肠道切除术(I²:82.8%)的肝硬化患者中(I²:89.3%)以及在技术复杂性方面(最复杂的LLR的I²:84.1%)。这些方面在总体发病率(I²:84.9%)、住院时间延长(I²:86.9%)和中转率(I²:73.4%)方面导致了实质性或较大的异质性。主要并发症具有中等异质性(I²:46.5%)。死亡率的异质性为零。风险调整解释了所有这些变异性,最终风险标准化中转率为8.9%,总体发病率为22.1%,主要发病率为5.1%,住院时间延长为26.0%。41个参与中心中没有异常值。提供了一个在线工具。
提供了包括所有符合条件患者的LLR基准,表明外科医生可以为了患者的利益采取相应行动,根据不同的适应证和不同的经验调整他们的手术方法,但最终提供相同质量的医疗服务。