Department of Cardiology, National Hospital Organization Kyoto Medical Center, 1-1, Mukaihata-cho, Fukakusa, Fushimi-ku, Kyoto, 612-8555, Japan.
Department of Nursing, National Hospital Organization Kyoto Medical Center, Kyoto, Japan.
ESC Heart Fail. 2022 Jun;9(3):1963-1975. doi: 10.1002/ehf2.13907. Epub 2022 Mar 20.
Patients with heart failure (HF) may have variable unrecognized symptom burdens. We sought to investigate the details, determinants, and prognostic significance of symptom burden in hospitalized patients with HF.
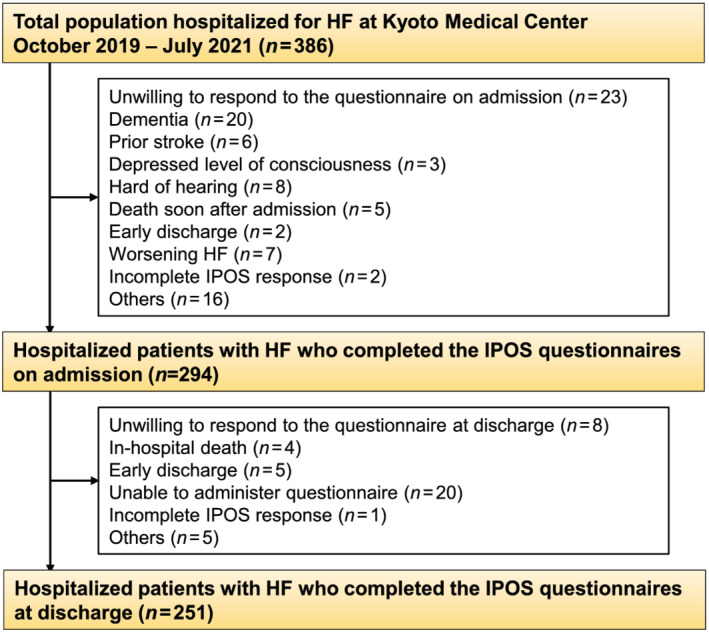
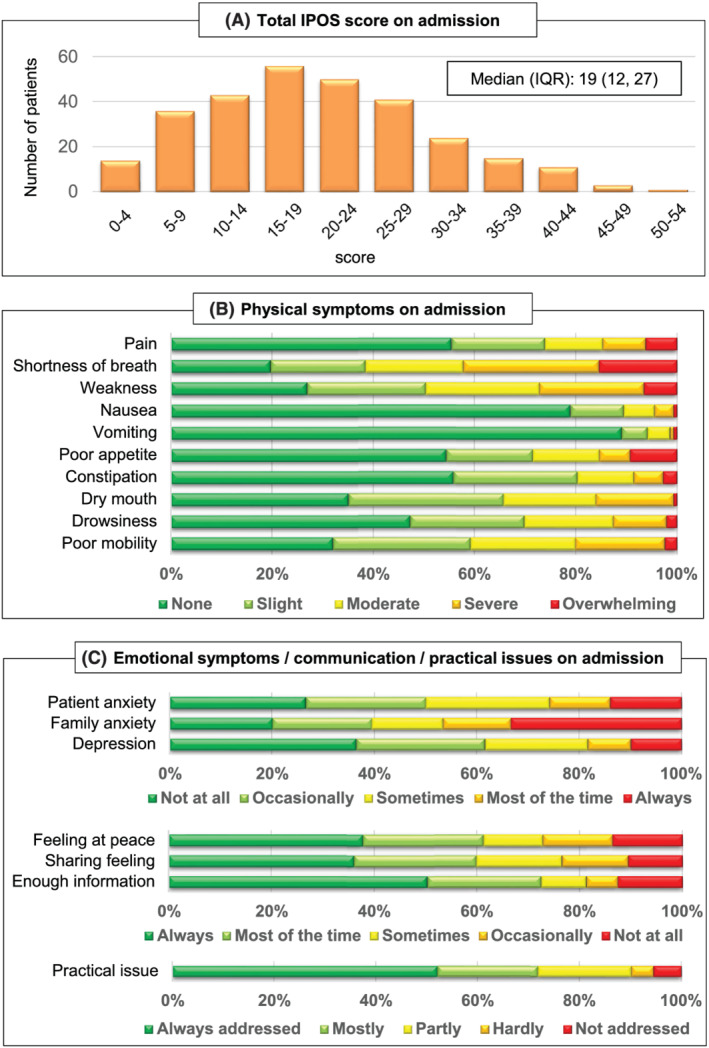
We prospectively evaluated consecutive hospitalized patients with HF as primary diagnosis at our institution using the Integrated Palliative care Outcome Scale (IPOS) both on admission and at discharge. The IPOS, which is a well-validated multi-dimensional symptom assessment scale among advanced illness, consists of 17 questions for enquiring about physical symptoms (10 items), emotional symptoms (4 items) and communication and practical issues (3 items) using a 5-point Likert scale (0 [best]-4 [worst] points). Clinically relevant symptoms were defined as ≥2 points for each IPOS item. Worsening symptom burden was defined as the total IPOS score at discharge being poorer than that on admission. Of 294 patients (mean age: 77.5 ± 12.0 years, male: 168 patients, New York Heart Association class IV: 96 patients, mean left ventricular ejection fraction [LVEF]: 44%, and median N-terminal pro B-type natriuretic peptide [NT-proBNP] level: 4418 ng/L), the median (IQR) total IPOS score on admission was 19 (12, 27) and they were widely distributed (minimum: 0 - maximum: 52). The total IPOS score on admission was not correlated with the HF severity, including LVEF (Spearman's ρ = -0.05, P = 0.43), NT-proBNP levels (Spearman's ρ = 0.08, P = 0.20) or in-hospital mortality prediction model (GWTG-HF risk score) (Spearman's ρ = 0.01, P = 0.90). Total IPOS scores significantly decreased during hospitalization as a whole (median [IQR]: 13 [6, 21] at discharge; P < 0.001 vs. those on admission). All of the four emotional symptoms (patient anxiety, depression, family anxiety and feeling at peace) remained in the top 5 of clinically relevant symptoms at discharge, whereas none of 10 physical symptoms were nominated. Worsening symptom burden was noted in 28% of the patients during hospitalization, and was independently associated with higher all-cause mortality after discharge (hazard ratio: 2.28, 95% confidence interval: 1.02-5.09; P = 0.044) even after adjustment by age and HF mortality prediction model (MAGGIC risk score).
We revealed that hospitalized patients with HF had multi-dimensional symptom burdens which varied among individuals and were not correlated with the disease severity. Emotional symptoms, such as anxiety and depression, were the main clinically relevant symptoms at discharge. A worsening IPOS score was noted in a quarter of patients with HF and was associated with a poor prognosis, suggesting the importance of holistic symptom assessment during the course of hospitalization for HF.
心力衰竭(HF)患者可能存在不同程度的未被识别的症状负担。我们旨在调查住院 HF 患者症状负担的详细情况、决定因素和预后意义。
我们前瞻性地评估了我院因 HF 住院的连续患者,使用综合姑息治疗结局量表(IPOS)在入院和出院时进行评估。IPOS 是一种在晚期疾病中经过良好验证的多维症状评估量表,包含 17 个问题,用于询问身体症状(10 项)、情绪症状(4 项)和沟通及实际问题(3 项),采用 5 分 Likert 量表(0[最佳]-4[最差]分)。临床相关症状定义为每个 IPOS 项目的评分≥2 分。症状负担恶化定义为出院时的总 IPOS 评分比入院时更差。在 294 名患者(平均年龄:77.5±12.0 岁,男性:168 名,纽约心脏协会心功能分级 IV 级:96 名,平均左心室射血分数[LVEF]:44%,中位数 N 末端脑钠肽前体[NT-proBNP]水平:4418ng/L)中,入院时的中位数(IQR)总 IPOS 评分为 19(12,27),分布广泛(最小值:0-最大值:52)。入院时的总 IPOS 评分与 HF 严重程度无关,包括 LVEF(Spearman ρ=−0.05,P=0.43)、NT-proBNP 水平(Spearman ρ=0.08,P=0.20)或院内死亡预测模型(GWTG-HF 风险评分)(Spearman ρ=0.01,P=0.90)。总体而言,住院期间 IPOS 评分显著下降(中位数[IQR]:出院时 13[6,21];P<0.001 与入院时相比)。在出院时,所有 4 项情绪症状(患者焦虑、抑郁、家属焦虑和内心平静)仍然是前 5 位的临床相关症状,而 10 项身体症状均未被提名。在住院期间,28%的患者出现症状负担恶化,出院后全因死亡率更高(风险比:2.28,95%置信区间:1.02-5.09;P=0.044),即使在调整年龄和 HF 死亡预测模型(MAGGIC 风险评分)后也是如此。
我们发现 HF 住院患者存在多维症状负担,个体间存在差异,与疾病严重程度无关。焦虑和抑郁等情绪症状是出院时的主要临床相关症状。HF 患者中有四分之一出现 IPOS 评分恶化,与预后不良相关,提示在 HF 住院期间进行整体症状评估的重要性。