Division of Nephrology, Kidney Research Institute, State Key Laboratory of Biotherapy and Cancer Center, West China Hospital, Sichuan University, Chengdu, 610041, China.
West China Biomedical Big Data Center, West China Hospital, Sichuan University, Guo Xue Lane 37, Chengdu, 610041, China.
BMC Med. 2022 Mar 22;20(1):94. doi: 10.1186/s12916-022-02289-1.
To elucidate the influence of childhood asthma on adult height after consideration of genetic heterogeneity in height.
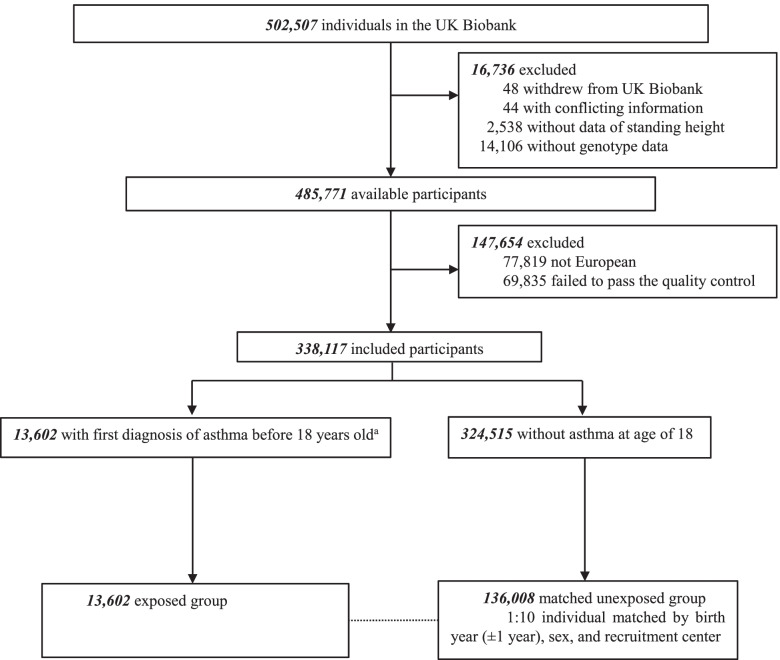
Based on the UK Biobank, we conducted a matched cohort study, including 13,602 European individuals with asthma diagnosed before 18 years old and 136,008 matched unexposed individuals without such an experience. Ascertainment of asthma was based on self-reported data (97.6%) or clinical diagnosis in healthcare registers (2.4%). We studied three height outcomes, including (1) the attained adult height (in centimeters), (2) the height deviation measured as the difference between a person's rank of genetically determined height (based on generated polygenetic risk score) and their rank of attained adult height in the study population (deviation in % of height order after standardization), and (3) the presence of height deficit comparing genetically determined and attained height (yes or no). We applied linear mixed-effect models to assess the associations of asthma diagnosed at different ages with attained adult height and height deviation, and conditional logistic regression models to estimate the associations of asthma with the risk of height deficit.
40.07% (59,944/149,610) of the study participants were born before 1950, and most of them were men (57.65%). After controlling for multiple covariates, childhood asthma was associated with shorter attained adult height, irrespective of age at asthma diagnosis. However, in the analysis of height deviation (deviation in %), we observed the greatest height deviation among individuals with asthma diagnosed before 4 years of age (- 2.57 [95% CI - 4.14 to - 1.00] and - 2.80 [95% CI - 4.06 to - 1.54] for the age of ≤ 2 and 3-4 years, respectively). The magnitude of height deviation in relation to asthma declined thereafter and became null after age 6. Similarly, there was a statistically significant height deficit in relation to an asthma diagnosis at ages ≤ 2 and 3-4 (odds ratios = 1.21, 95% CI 1.04 to 1.40, and 1.15, 95% CI 1.02 to 1.29) but not thereafter. The result pattern was similar when separately analyzing asthma with or without inhaled glucocorticoid (ICS) use, despite that the estimates were consistently stronger among asthma individuals who used ICS.
Our results suggest a notable association of childhood asthma, primarily asthma diagnosed at an early age, with adult height, after consideration of genetic heterogeneity in height and use of ICS. This finding highlights the need for surveillance on the growth problems among children with asthma.
为了阐明考虑身高遗传异质性后,儿童哮喘对成年身高的影响。
基于英国生物库,我们进行了一项匹配队列研究,纳入了 13602 名在 18 岁之前被诊断为哮喘的欧洲个体和 136008 名未暴露于哮喘的匹配个体。哮喘的确定基于自我报告数据(97.6%)或医疗保健登记处的临床诊断(2.4%)。我们研究了三种身高结果,包括(1)成年时的实际身高(厘米),(2)身高偏差,定义为个体基于生成的多基因风险评分的遗传决定身高等级与其在研究人群中的成年实际身高等级之间的差异(标准化后身高等级的偏差%),(3)比较遗传决定身高和实际身高的身高不足的存在(是或否)。我们应用线性混合效应模型评估不同年龄诊断的哮喘与成年时实际身高和身高偏差的关系,并应用条件逻辑回归模型估计哮喘与身高不足风险的关系。
研究参与者中 40.07%(59944/149610)出生于 1950 年之前,且大多数为男性(57.65%)。在控制了多个协变量后,儿童时期的哮喘与成年时的实际身高较矮有关,无论哮喘的诊断年龄如何。然而,在身高偏差(偏差%)的分析中,我们观察到在 4 岁之前被诊断出哮喘的个体中身高偏差最大(年龄≤2 岁时为-2.57[95%置信区间-4.14 至-1.00],年龄 3-4 岁时为-2.80[95%置信区间-4.06 至-1.54])。此后,与哮喘相关的身高偏差幅度下降,6 岁后则变得无关紧要。同样,在年龄≤2 岁和 3-4 岁时诊断出哮喘与身高不足存在统计学显著关联(比值比=1.21,95%置信区间 1.04 至 1.40,和 1.15,95%置信区间 1.02 至 1.29),但此后则无关紧要。当分别分析有或无吸入性糖皮质激素(ICS)使用的哮喘时,结果模式相似,尽管在使用 ICS 的哮喘个体中,估计值始终更强。
我们的结果表明,儿童哮喘,尤其是早期诊断的哮喘,与成年身高显著相关,这是在考虑身高遗传异质性和 ICS 使用的情况下得出的。这一发现强调了需要监测哮喘儿童的生长问题。