Evidera, London, UK.
Division of Epidemiology, Department of Quantitative Health Sciences, Mayo Clinic, Rochester, Minnesota, USA.
Cancer Med. 2022 Aug;11(16):3156-3167. doi: 10.1002/cam4.4678. Epub 2022 Mar 21.
Guidelines include several options for average-risk colorectal cancer (CRC) screening that vary in aspects such as invasiveness, recommended frequency, and precision. Thus, patient and provider preferences can help identify an appropriate screening strategy. This study elicited CRC screening preferences of physicians and individuals at average risk for CRC (IAR).
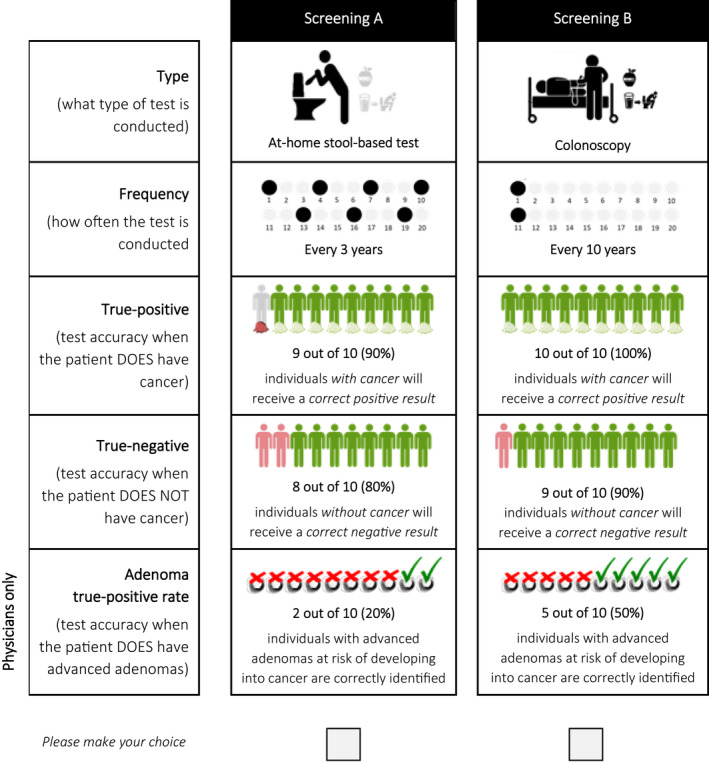
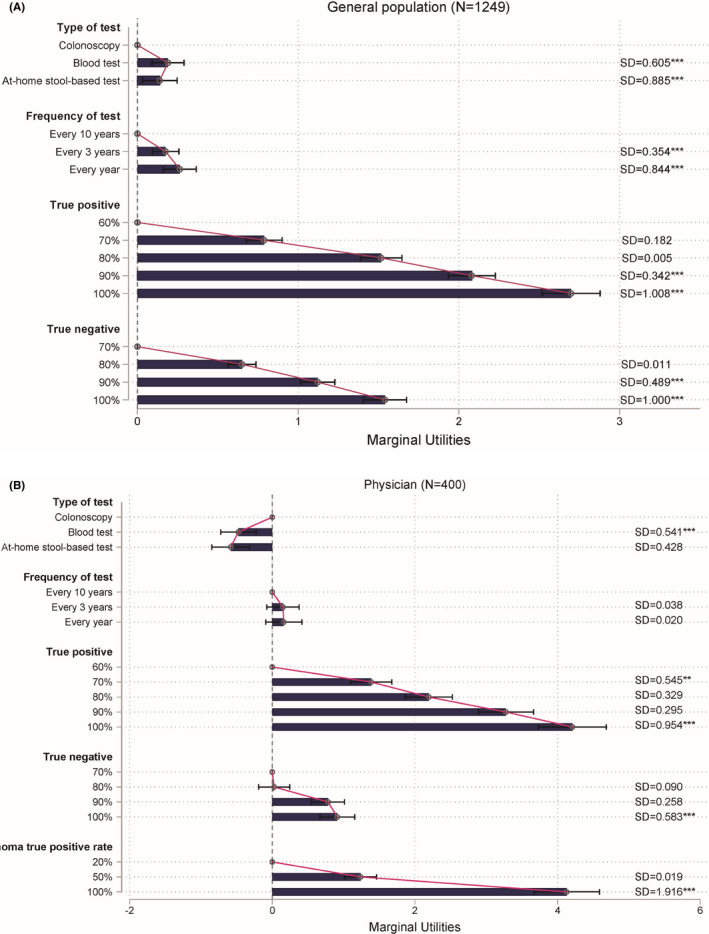
IAR aged 45-75 years and licensed physicians (primary care or gastroenterology) completed an online discrete choice experiment (DCE). Participants were recruited from representative access panels in the US. Within the DCE, participants traded off preferences between screening type, screening frequency, true-positive, true-negative, and adenoma true positive (physicians only). A mixed logit model was used to obtain predicted choice probabilities for colonoscopy, multi-target stool DNA (mt-sDNA), fecal immunochemical test (FIT), and methylated septin 9 (mSEPT9) blood test.
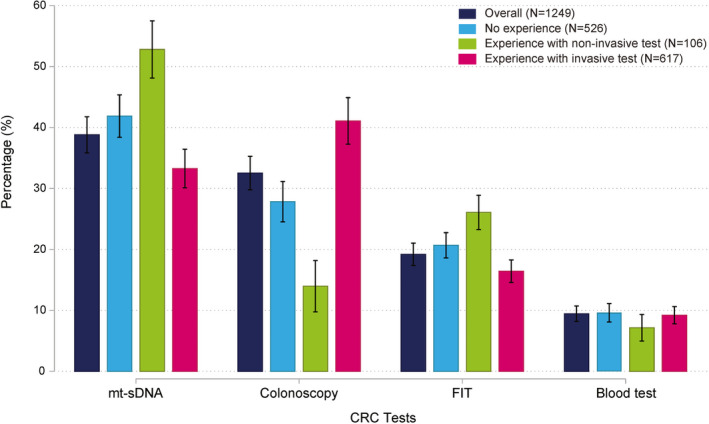
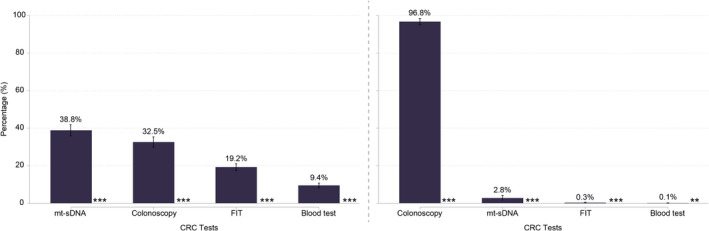
Preferences of IAR and physicians were affected by screening precision and screening type. IAR also valued more regular screening. Physicians preferred colonoscopy (96.8%) over mt-sDNA (2.8%; p < 0.001), FIT (0.3%; p < 0.001) and mSEPT9 blood test (0.1%; p < 0.01). IAR preferred mt-sDNA (38.8%) over colonoscopy (32.5%; p < 0.001), FIT (19.2%; p < 0.001), and mSEPT9 blood test (9.4%; p < 0.001). IAR naïve to screening preferred non-invasive screening (p < 0.001), while the opposite was found for those who previously underwent colonoscopy or sigmoidoscopy.
While physicians overwhelmingly preferred colonoscopy, preferences of IAR were heterogenous, with mt-sDNA being most frequently preferred on average. Offering choices in addition to colonoscopy could improve CRC screening uptake among IAR. This study used a discrete choice experiment in the US to elicit preferences of physicians and individuals at average risk for colorectal cancer screening modalities and their characteristics.
指南中包含了几种针对结直肠癌(CRC)筛查的选择,这些选择在侵袭性、推荐频率和准确性等方面存在差异。因此,患者和提供者的偏好可以帮助确定合适的筛查策略。本研究旨在了解普通风险结直肠癌(CRC)患者(IAR)和医生对 CRC 筛查的偏好。
年龄在 45-75 岁之间的 IAR 和持照医生(初级保健或胃肠病学)完成了在线离散选择实验(DCE)。参与者是从美国具有代表性的准入小组中招募的。在 DCE 中,参与者根据筛查类型、筛查频率、真阳性、真阴性和腺瘤真阳性(仅限医生)对偏好进行权衡。使用混合对数模型获得结肠镜检查、多靶点粪便 DNA(mt-sDNA)、粪便免疫化学试验(FIT)和甲基化 Septin 9(mSEPT9)血液检测的预测选择概率。
IAR 和医生的偏好受筛查精度和筛查类型的影响。IAR 还更看重更定期的筛查。医生更倾向于结肠镜检查(96.8%)而不是 mt-sDNA(2.8%;p<0.001)、FIT(0.3%;p<0.001)和 mSEPT9 血液检测(0.1%;p<0.01)。IAR 更倾向于 mt-sDNA(38.8%)而不是结肠镜检查(32.5%;p<0.001)、FIT(19.2%;p<0.001)和 mSEPT9 血液检测(9.4%;p<0.001)。对筛查不熟悉的 IAR 更喜欢非侵入性筛查(p<0.001),而对于那些之前接受过结肠镜检查或乙状结肠镜检查的人则相反。
虽然医生普遍倾向于结肠镜检查,但 IAR 的偏好存在异质性,平均而言,mt-sDNA 是最常被选择的。在结肠镜检查之外提供选择可以提高 IAR 对 CRC 筛查的接受度。本研究使用离散选择实验在美国调查了医生和普通风险结直肠癌筛查模式及其特征的个体的偏好。