National Cancer Center Hospital East, Kashiwa, Japan.
The University of Texas MD Anderson Cancer Center, Houston, TX, USA.
Nature. 2022 Mar;603(7903):942-948. doi: 10.1038/s41586-022-04508-4. Epub 2022 Mar 23.
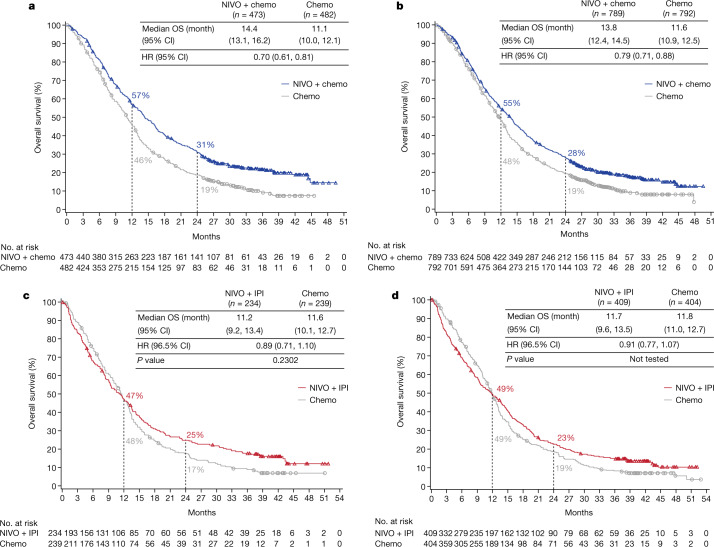
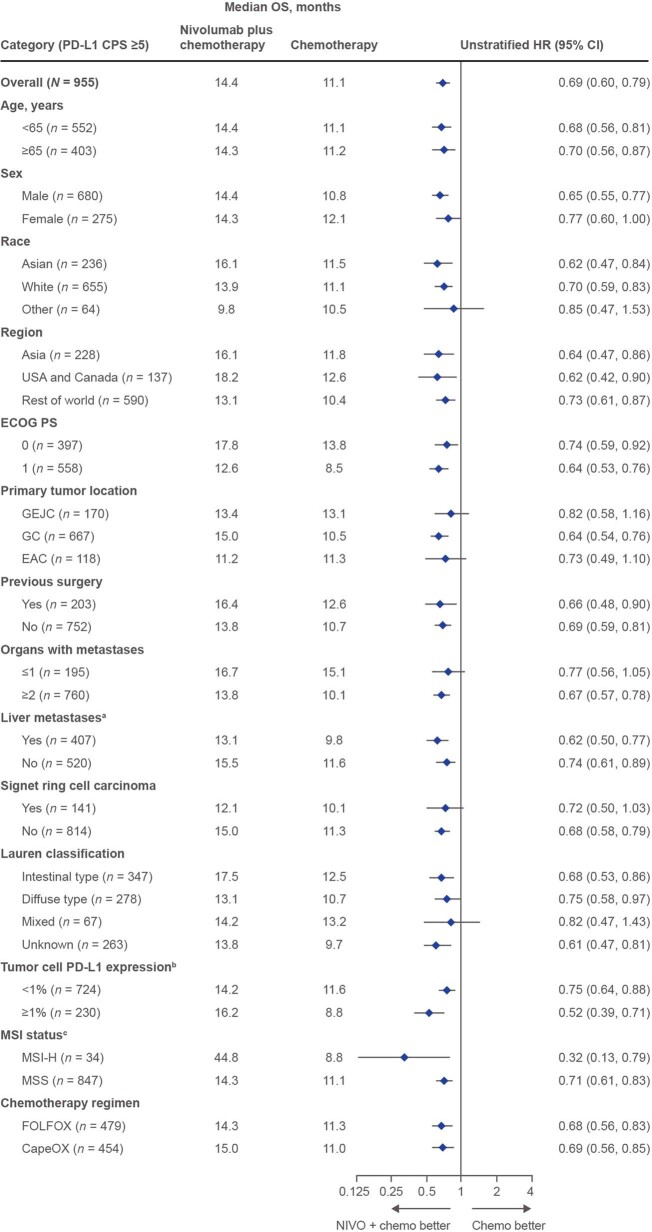
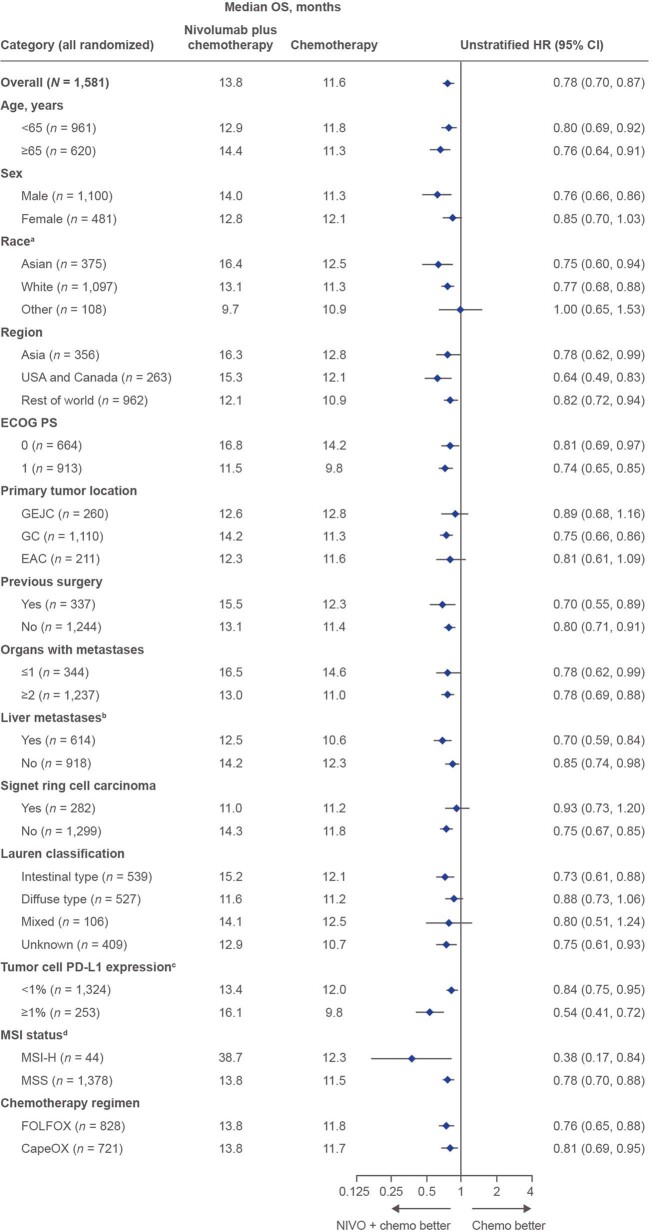
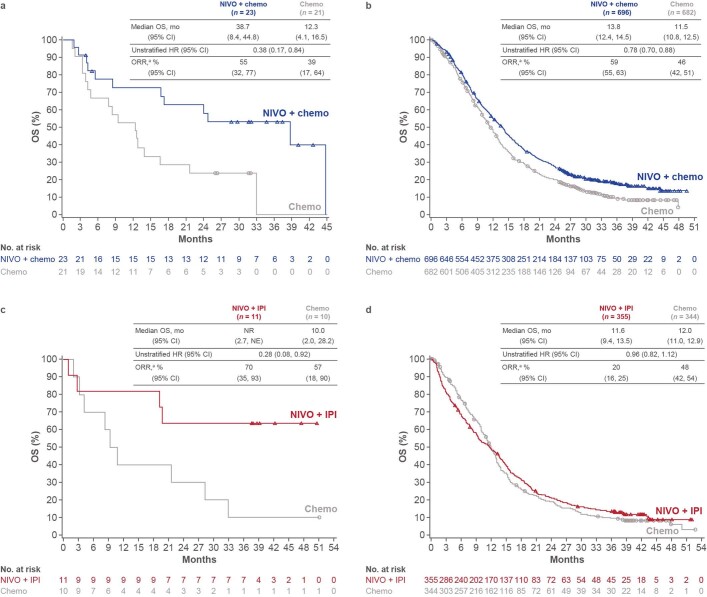
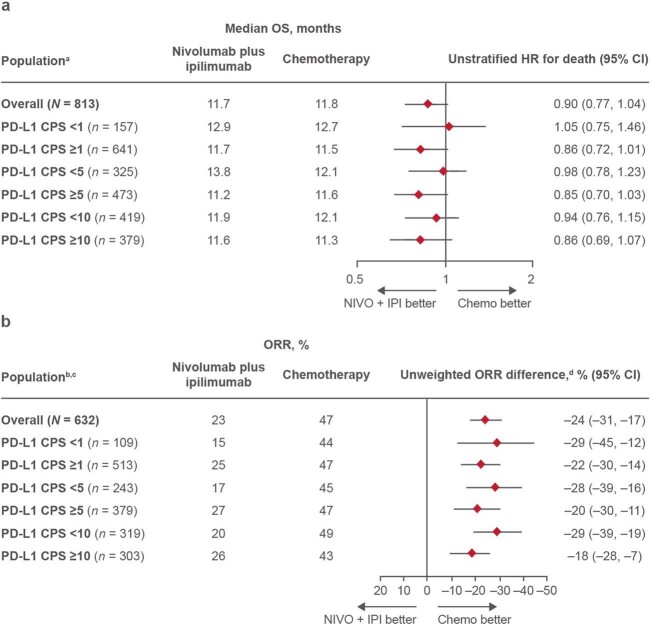
Standard first-line chemotherapy results in disease progression and death within one year in most patients with human epidermal growth factor receptor 2 (HER2)-negative gastro-oesophageal adenocarcinoma. Nivolumab plus chemotherapy demonstrated superior overall survival versus chemotherapy at 12-month follow-up in gastric, gastro-oesophageal junction or oesophageal adenocarcinoma in the randomized, global CheckMate 649 phase 3 trial (programmed death ligand-1 (PD-L1) combined positive score ≥5 and all randomized patients). On the basis of these results, nivolumab plus chemotherapy is now approved as a first-line treatment for these patients in many countries. Nivolumab and the cytotoxic T-lymphocyte antigen-4 (CTLA-4) inhibitor ipilimumab have distinct but complementary mechanisms of action that contribute to the restoration of anti-tumour T-cell function and induction of de novo anti-tumour T-cell responses, respectively. Treatment combining 1 mg kg nivolumab with 3 mg kg ipilimumab demonstrated clinically meaningful anti-tumour activity with a manageable safety profile in heavily pre-treated patients with advanced gastro-oesophageal cancer. Here we report both long-term follow-up results comparing nivolumab plus chemotherapy versus chemotherapy alone and the first results comparing nivolumab plus ipilimumab versus chemotherapy alone from CheckMate 649. After the 24.0-month minimum follow-up, nivolumab plus chemotherapy continued to demonstrate improvement in overall survival versus chemotherapy alone in patients with PD-L1 combined positive score ≥5 (hazard ratio 0.70; 95% confidence interval 0.61, 0.81) and all randomized patients (hazard ratio 0.79; 95% confidence interval 0.71, 0.88). Overall survival in patients with PD-L1 combined positive score ≥ 5 for nivolumab plus ipilimumab versus chemotherapy alone did not meet the prespecified boundary for significance. No new safety signals were identified. Our results support the continued use of nivolumab plus chemotherapy as standard first-line treatment for advanced gastro-oesophageal adenocarcinoma.
在大多数人表皮生长因子受体 2(HER2)阴性胃食管腺癌患者中,标准一线化疗在一年内导致疾病进展和死亡。在全球随机 CheckMate 649 三期临床试验(程序性死亡配体-1(PD-L1)联合阳性评分≥5 和所有随机患者)中,纳武利尤单抗联合化疗在胃、胃食管交界处或食管腺癌患者中与化疗相比,在 12 个月随访时显示出总生存期优势(程序死亡配体-1(PD-L1)联合阳性评分≥5 和所有随机患者)。基于这些结果,纳武利尤单抗联合化疗现在在许多国家被批准用于这些患者的一线治疗。纳武利尤单抗和细胞毒性 T 淋巴细胞相关抗原 4(CTLA-4)抑制剂伊匹单抗具有不同但互补的作用机制,分别有助于恢复抗肿瘤 T 细胞功能和诱导新的抗肿瘤 T 细胞反应。在晚期胃食管癌中,治疗方案为 1mg/kg 纳武利尤单抗联合 3mg/kg 伊匹单抗,结果显示出具有临床意义的抗肿瘤活性,安全性可控。在此,我们报告了 CheckMate 649 中比较纳武利尤单抗联合化疗与单纯化疗的长期随访结果,以及比较纳武利尤单抗联合伊匹单抗与单纯化疗的首次结果。在 24.0 个月的最小随访后,在 PD-L1 联合阳性评分≥5(风险比 0.70;95%置信区间 0.61,0.81)和所有随机患者(风险比 0.79;95%置信区间 0.71,0.88)中,纳武利尤单抗联合化疗继续显示出与单纯化疗相比的总生存改善。纳武利尤单抗联合伊匹单抗与单纯化疗相比,在 PD-L1 联合阳性评分≥5 的患者中,总生存未达到预设的显著性边界。没有发现新的安全性信号。我们的结果支持继续使用纳武利尤单抗联合化疗作为晚期胃食管腺癌的标准一线治疗。