Baldo Brian A
Kolling Institute of Medical Research, Royal North Shore Hospital of Sydney, Sydney, NSW 2065, Australia.
Department of Medicine, University of Sydney, Sydney, NSW 2065, Australia.
Antibodies (Basel). 2022 Feb 25;11(1):17. doi: 10.3390/antib11010017.
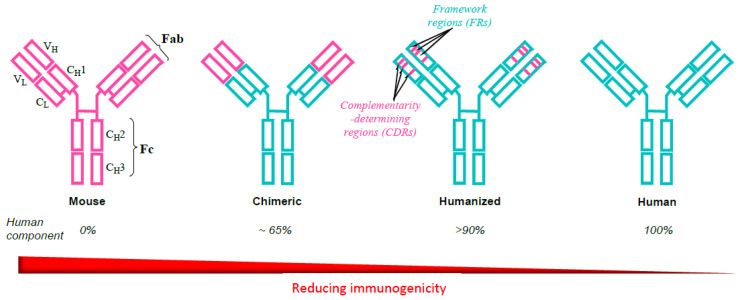
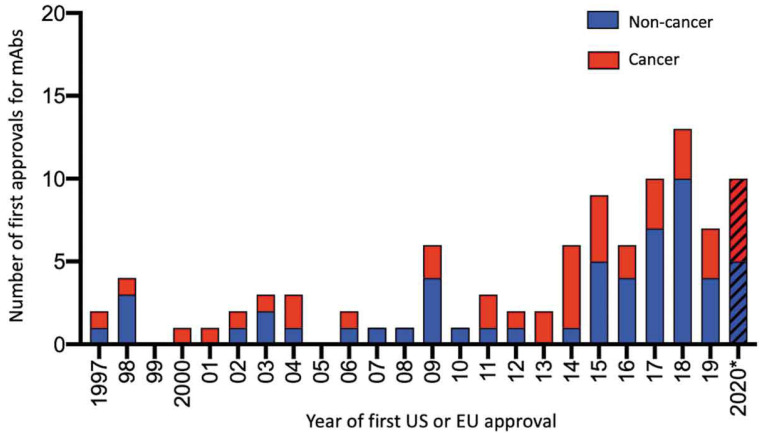
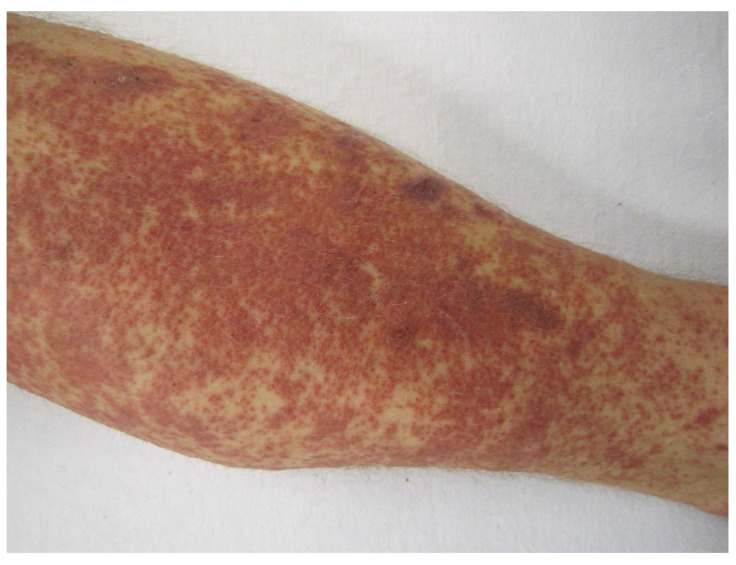
Identification of new disease-associated biomarkers; specific targeting of such markers by monoclonal antibodies (mAbs); and application of advances in recombinant technology, including the production of humanized and fully human antibodies, has enabled many improved treatment outcomes and successful new biological treatments of some diseases previously neglected or with poor prognoses. Of the 110 mAbs preparations currently approved by the FDA and/or EMA, 46 (including 13 antibody-drug conjugates) recognizing 29 different targets are indicated for the treatment of cancers, and 66, recognizing 48 different targets, are indicated for non-cancer disorders. Despite their specific targeting with the expected accompanying reduced collateral damage for normal healthy non-involved cells, mAbs, may cause types I (anaphylaxis, urticaria), II (e.g., hemolytic anemia, possibly early-onset neutropenia), III (serum sickness, pneumonitis), and IV (Stevens-Johnson syndrome, toxic epidermal necrolysis) hypersensitivities as well as other cutaneous, pulmonary, cardiac, and liver adverse events. MAbs can provoke severe infusion reactions that resemble anaphylaxis and induce a number of systemic, potentially life-threatening syndromes with low frequency. A common feature of most of these syndromes is the release of a cascade of cytokines associated with inflammatory and immunological processes. Epidermal growth factor receptor-targeted antibodies may provoke papulopustular and mucocutaneous eruptions that are not immune-mediated.
新型疾病相关生物标志物的鉴定;通过单克隆抗体(mAb)对这些标志物进行特异性靶向;以及重组技术进展的应用,包括人源化抗体和全人源抗体的生产,已带来了许多更好的治疗效果,并成功实现了对一些先前被忽视或预后不良疾病的新型生物治疗。在美国食品药品监督管理局(FDA)和/或欧洲药品管理局(EMA)目前批准的110种mAb制剂中,有46种(包括13种抗体药物偶联物)可识别29个不同靶点,用于治疗癌症;66种可识别48个不同靶点,用于治疗非癌症疾病。尽管mAb具有特异性靶向作用,预期对正常健康未受累细胞的附带损害会减少,但它们可能会引发I型(过敏反应、荨麻疹)、II型(例如溶血性贫血、可能的早发性中性粒细胞减少症)、III型(血清病、肺炎)和IV型(史蒂文斯-约翰逊综合征、中毒性表皮坏死松解症)超敏反应以及其他皮肤、肺部、心脏和肝脏不良事件。mAb可引发类似于过敏反应的严重输液反应,并以低频率诱发一些全身性、潜在危及生命的综合征。这些综合征大多数的一个共同特征是与炎症和免疫过程相关的一系列细胞因子的释放。靶向表皮生长因子受体的抗体可能会引发丘疹脓疱性和黏膜皮肤疹,这些皮疹并非免疫介导的。