Department of Internal Medicine, University of Manitoba, Winnipeg, Manitoba, Canada.
School of Public Health Sciences, University of Waterloo, Waterloo, Ontario, Canada.
Age Ageing. 2022 Mar 1;51(3). doi: 10.1093/ageing/afac049.
Nursing home (NH) residents should have the opportunity to consider, discuss and document their healthcare wishes. However, such advance care planning (ACP) is frequently suboptimal.
Assess a comprehensive, person-centred ACP approach.
Unblinded, cluster randomised trial.
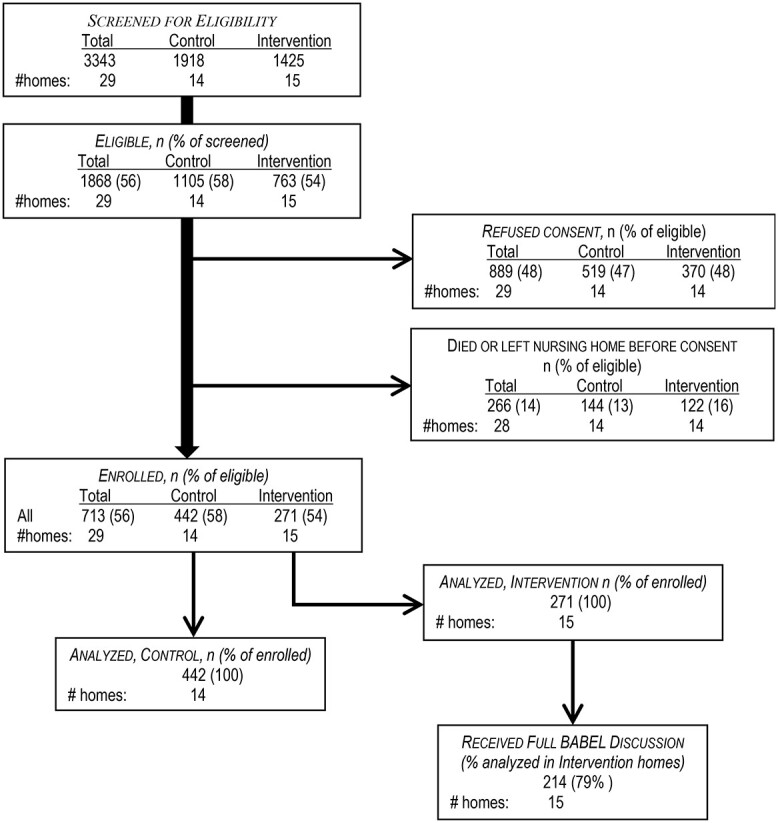
Fourteen control and 15 intervention NHs in three Canadian provinces, 2018-2020.
713 residents (442 control, 271 intervention) aged ≥65 years, with elevated mortality risk.
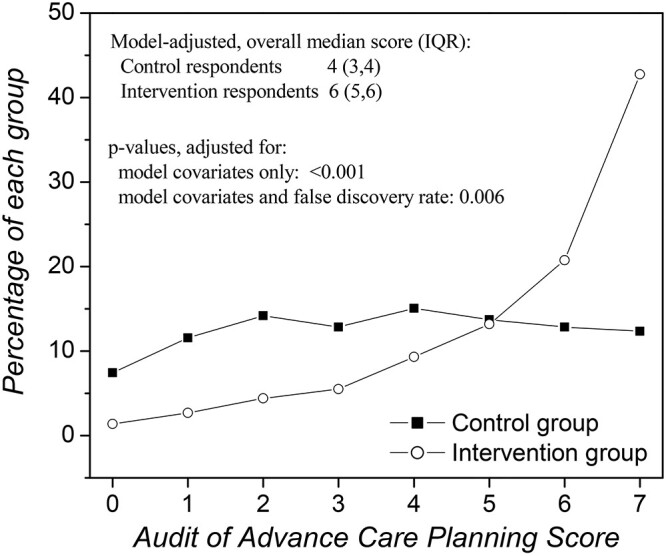
The intervention was a structured, $\sim$60-min discussion between a resident, substitute decision-maker (SDM) and nursing home staff to: (i) confirm SDMs' identities and role; (ii) prepare SDMs for medical emergencies; (iii) explain residents' clinical condition and prognosis; (iv) ascertain residents' preferred philosophy to guide decision-making and (v) identify residents' preferred options for specific medical emergencies. Control NHs continued their usual ACP processes. Co-primary outcomes were: (a) comprehensiveness of advance care planning, assessed using the Audit of Advance Care Planning, and (b) Comfort Assessment in Dying. Ten secondary outcomes were assessed. P-values were adjusted for all 12 outcomes using the false discovery rate method.
The intervention resulted in 5.21-fold higher odds of respondents rating ACP comprehensiveness as being better (95% confidence interval [CI] 3.53, 7.61). Comfort in dying did not differ (difference = -0.61; 95% CI -2.2, 1.0). Among the secondary outcomes, antimicrobial use was significantly lower in intervention homes (rate ratio = 0.79, 95% CI 0.66, 0.94).
Superior comprehensiveness of the BABEL approach to ACP underscores the importance of allowing adequate time to address all important aspects of ACP and may reduce unwanted interventions towards the end of life.
养老院(NH)居民应有机会考虑、讨论和记录他们的医疗意愿。然而,这种预先医疗指示(ACP)通常并不理想。
评估一种全面的、以患者为中心的 ACP 方法。
非盲、集群随机试验。
2018 年至 2020 年,在加拿大三个省份的 14 个对照和 15 个干预 NH。
713 名年龄≥65 岁、死亡率较高的居民(442 名对照,271 名干预)。
干预措施是居民、替代决策者(SDM)和养老院工作人员之间进行的一次结构化的、大约 60 分钟的讨论,内容包括:(i)确认 SDM 的身份和角色;(ii)使 SDM 为医疗紧急情况做好准备;(iii)解释居民的临床状况和预后;(iv)确定居民偏好的指导决策的哲学;以及(v)确定居民对特定医疗紧急情况的偏好选择。对照 NH 继续进行其常规的 ACP 流程。主要结局指标为:(a)使用预先医疗指示审计评估预先医疗指示计划的全面性,以及(b)临终舒适度。评估了 10 个次要结局指标。所有 12 个结局指标的 P 值均使用错误发现率方法进行了调整。
干预组受访者对 ACP 全面性的评分更好的可能性高出 5.21 倍(95%置信区间[CI] 3.53,7.61)。临终舒适度没有差异(差值=-0.61;95% CI -2.2,1.0)。在次要结局中,干预组的抗菌药物使用率显著降低(率比=0.79,95% CI 0.66,0.94)。
BABEL 方法在 ACP 方面的优越性表明,充分的时间来解决 ACP 的所有重要方面非常重要,并且可能会减少生命末期不必要的干预。