Clinical Institute for Special Laboratory Diagnostics, University Children's Hospital, UMC Ljubljana, 1000 Ljubljana, Slovenia.
Department of Endocrinology, Diabetes and Metabolic Diseases, University Children's Hospital, UMC Ljubljana, 1000 Ljubljana, Slovenia.
Genes (Basel). 2022 Mar 15;13(3):517. doi: 10.3390/genes13030517.
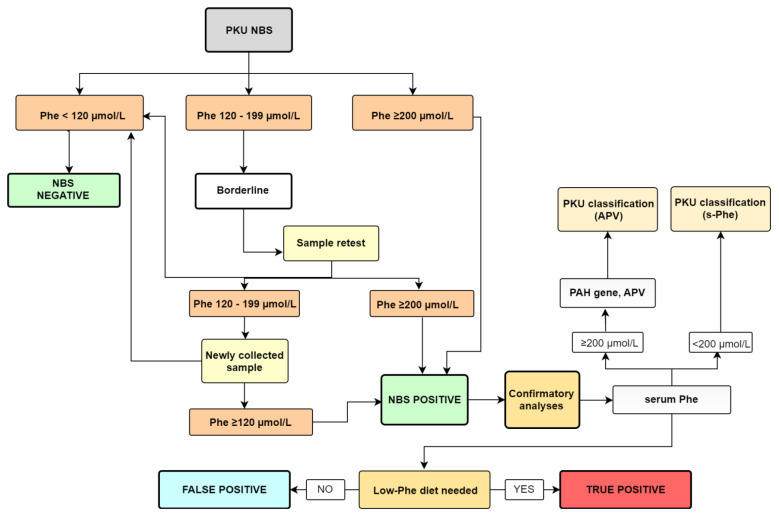
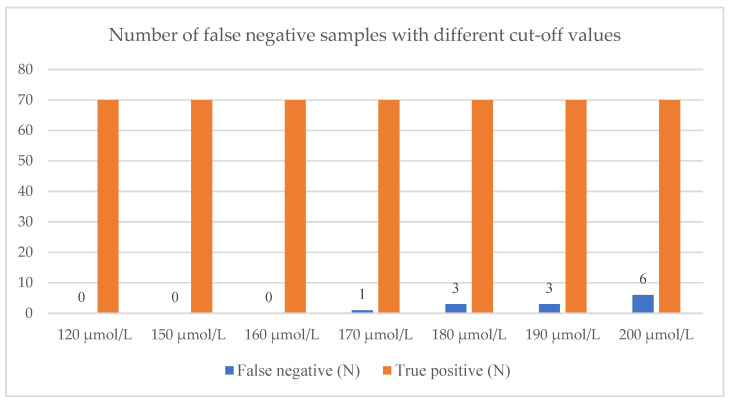
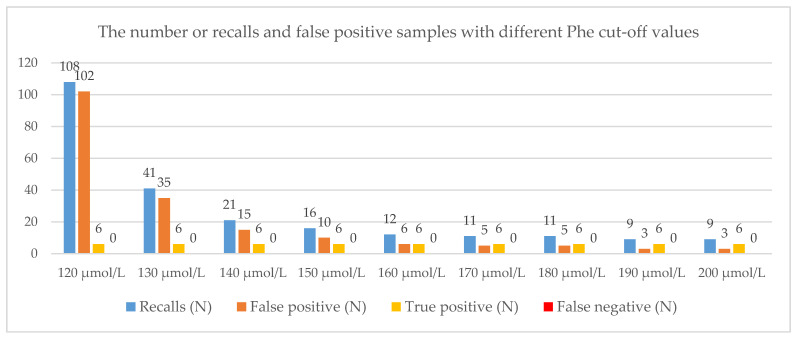
Phenylketonuria (PKU) was the first disorder for which newborn screening (NBS) was introduced in the early 1960s. Slovenia started the NBS program for PKU in 1979, and the fluorimetric method was implemented in 1992, with a phenylalanine (Phe) cut-off set at 120 mol/L. This value has been in use for almost thirty years and has never been revised. We aimed to analyze the DBS samples and review the data from a large nationwide cohort of newborns to optimize the cut-off values for HFA screening to minimize the number of false positives while maintaining the highest level of sensitivity by detecting all those who needed to be treated. In the first prospective part of the study, we analyzed samples of all newborns in Slovenia in 2019 and 2020, and in the second retrospective part, we reviewed data from all known patients with hyperphenylalaninemia (HFA) in Slovenia born from 2000 to 2018. We defined true screening-positive cases as those that required a low-Phe diet. The sensitivity, specificity and positive predictive values of the modeling elevation of the Phe cut-off value from 120 µmol/L to 200 µmol/L were assessed. The number of recalls at the cut-off of 120 µmol/L was 108 out of 37,784 samples at NBS (2019-2020). Six newborns were defined as true positives and 102 samples as false positives. If the cut-off value was adjusted to 160 µmol/L, only 12 samples exceeded it and all six true positive newborns would be detected. Among the 360,000 samples collected at the NBS between 2000 and 2018, 72 HFA patients in need of a low-Phe diet were found. All the diagnosed cases would have been detected if the cut-off was set to 160 µmol/L. We demonstrated in a large group of newborns (400,000 in 20 years) that using the fluorimetric approach, a cut-off value of 160 µmol/L, rather than 120 mol/L, is safe and that there were no missing true positive patients who required treatment. By increasing the cut-off, this method becomes more precise, resulting in a significantly reduced rate of false positives and thus being less burdensome on both families and the healthcare system.
苯丙酮尿症(PKU)是 20 世纪 60 年代初引入新生儿筛查(NBS)的首个疾病。斯洛文尼亚于 1979 年启动了 PKU 的 NBS 计划,并于 1992 年实施了荧光法,苯丙氨酸(phe)截断值设定为 120 μmol/L。这一值已使用近三十年,从未修订过。我们旨在分析 DBS 样本,并回顾来自大型全国性新生儿队列的数据,以优化高苯丙氨酸血症(HFA)筛查的截断值,在通过检测所有需要治疗的患者来保持最高敏感度的同时,将假阳性数量降至最低。在研究的前瞻性第一部分,我们分析了 2019 年和 2020 年斯洛文尼亚所有新生儿的样本,在回顾性第二部分,我们回顾了 2000 年至 2018 年期间出生的所有已知 HFA 患者的数据。我们将真正的筛查阳性病例定义为需要低苯丙氨酸饮食的病例。评估了将phe 截断值从 120 μmol/L 升高到 200 μmol/L 的建模升高的敏感性、特异性和阳性预测值。在 NBS 中,120 μmol/L 截断值有 108 例召回,而 37784 例样本(2019-2020 年)。6 名新生儿被定义为真正的阳性,102 例样本为假阳性。如果将截断值调整为 160 μmol/L,则只有 12 例样本超过该值,并且所有 6 例真正的阳性新生儿都将被检测到。在 2000 年至 2018 年 NBS 收集的 36 万例样本中,发现了 72 例需要低苯丙氨酸饮食的 HFA 患者。如果将截断值设置为 160 μmol/L,所有确诊病例都将被检测到。我们在一大组新生儿(20 年内 40 万例)中证明,使用荧光法,截断值为 160 μmol/L,而不是 120 μmol/L,是安全的,并且没有遗漏需要治疗的真正阳性患者。通过提高截断值,该方法变得更加精确,从而显著降低假阳性率,从而减轻家庭和医疗保健系统的负担。