Katsanos Aristeidis H, Gupta Himanshu, Morotti Andrea, Beshara Simon, Patil Tushar, Al-Zahrani Saeed, Tsivgoulis Georgios, Dowlatshahi Dariush, Goldstein Joshua N, Charidimou Andreas, Shoamanesh Ashkan
Department of Medicine (Neurology), McMaster University/Population Health Research Institute, Hamilton, ON L8L2X2, Canada.
Department of Neurological Sciences and Vision, Neurology Unit, ASST Spedali Civili, 25123 Brescia, Italy.
J Clin Med. 2022 Mar 14;11(6):1596. doi: 10.3390/jcm11061596.
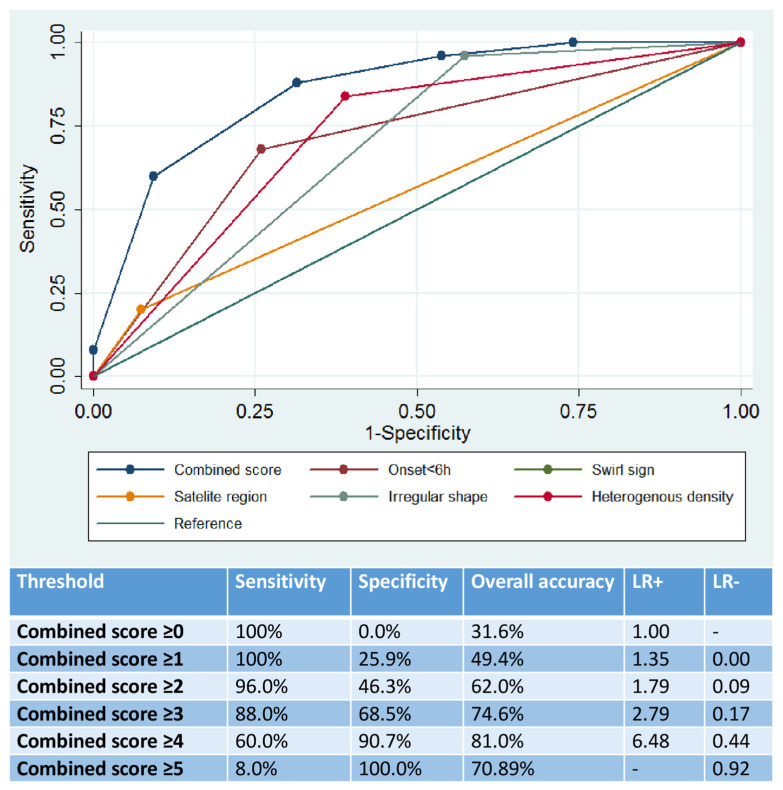
Background and aims: The utility of proposed non-contrast computed tomography (NCCT) markers for the prediction of hematoma expansion in patients with antithrombotic-related spontaneous intracerebral hemorrhage (ICH) is limited. Additionally, there is significant overlap between different suggested ICH shape and density markers. Methods: We assessed the prognostic yield for hematoma expansion of a combined score incorporating features of ICH shape irregularity (satellite sign and/or Barras score ≥ 3), heterogeneous ICH density (swirl sign and/or Barras score ≥ 3) on baseline NCCT and timing from ICH onset to NCCT. Results: We evaluated data from 79 patients with antithrombotic-related spontaneous ICH (32% with hematoma expansion). Swirl (84% vs. 39%) and satellite signs (20% vs. 7%) on baseline NCCT were significantly more prevalent (p < 0.001) in patients with hematoma expansion. Patients with hematoma expansion had more irregular and heterogeneous bleeds on baseline NCCT scans, as quantified by higher (p < 0.001) Barras shape (4 (4−5) vs. 3 (2−4)) and density scores (4 (3−5) vs. 2 (1−3)), respectively. The overall diagnostic yield of the combined score (area under the curve: 0.86, 95%CI: 0.78−0.94) significantly outperformed (p < 0.001) the diagnostic yield of each individual marker. Scores of 4 or 5 in the combined score were associated with a sensitivity of 60.0%, specificity of 90.7%, overall diagnostic accuracy of 81.0%, positive likelihood ratio (LR) of 6.48, negative LR of 0.44, positive predictive value (PV) of 0.76 and negative PV of 0.83. Conclusion: Combined NCCT marker assessment seems to increase the prognostic accuracy for hematoma expansion in antithrombotic-related spontaneous ICH patients.
用于预测抗栓相关自发性脑出血(ICH)患者血肿扩大的非增强计算机断层扫描(NCCT)标志物的效用有限。此外,不同的ICH形状和密度标志物之间存在显著重叠。方法:我们评估了一个综合评分对血肿扩大的预后价值,该评分纳入了基线NCCT上ICH形状不规则(卫星征和/或巴拉斯评分≥3)、ICH密度不均(漩涡征和/或巴拉斯评分≥3)的特征以及从ICH发作到NCCT的时间。结果:我们评估了79例抗栓相关自发性ICH患者的数据(32%有血肿扩大)。基线NCCT上的漩涡征(84%对39%)和卫星征(20%对7%)在血肿扩大的患者中显著更常见(p<0.001)。血肿扩大的患者在基线NCCT扫描上有更多不规则和不均匀的出血,分别通过更高的(p<0.001)巴拉斯形状评分(4(4 - 5)对3(2 - 4))和密度评分(4(3 - 5)对2(1 - 3))来量化。综合评分的总体诊断价值(曲线下面积:0.86,95%CI:0.78 - 0.94)显著优于(p<0.001)每个单独标志物的诊断价值。综合评分4分或5分的敏感性为60.0%,特异性为90.7%,总体诊断准确性为81.0%,阳性似然比(LR)为6.48,阴性LR为0.44,阳性预测值(PV)为0.76,阴性PV为0.83。结论:联合NCCT标志物评估似乎提高了抗栓相关自发性ICH患者血肿扩大的预后准确性。