RAND Corporation, 1776 Main Street, Santa Monica, CA, 90407, USA.
Centers for Medicare & Medicaid Services, Baltimore, MD, 21244, USA.
BMC Health Serv Res. 2022 Mar 24;22(1):388. doi: 10.1186/s12913-022-07743-7.
Most emergency department (ED) patients arrive by their own transport and, for various reasons, may not choose the nearest ED. How far patients travel for ED treatment may reflect both patients' access to care and severity of illness. In this study, we aimed to examine the travel distance and travel time between a patient's home and ED they visited and investigate how these distances/times vary by patient and hospital characteristics.
We randomly sampled and collected data from 14,812 patients discharged to the community (DTC) between January and March 2016 from 50 hospital-based EDs nationwide. We geocoded and calculated the distance and travel time between patient and hospital-based ED addresses, examined the travel distances/ times between patients' home and the ED they visited, and used mixed-effects regression models to investigate how these distances/times vary by patient and hospital characteristics.
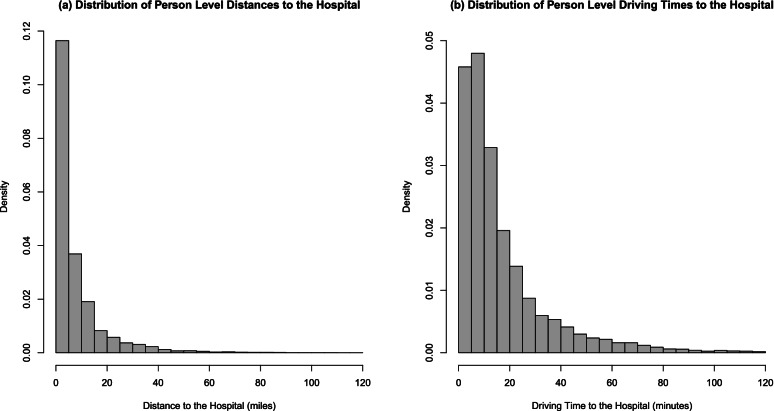
Patients travelled an average of 8.0 (SD = 10.9) miles and 17.3 (SD = 18.0) driving minutes to the ED. Patients travelled significantly farther to avoid EDs in lower performing hospitals (p < 0.01) and in the West (p < 0.05) and Midwest (p < 0.05). Patients travelled farther when visiting EDs in rural areas. Younger patients travelled farther than older patients.
Understanding how far patients are willing to travel is indicative of whether patient populations have adequate access to ED services. By showing that patients travel farther to avoid a low-performing hospital, we provide evidence that DTC patients likely do exercise some choice among EDs, indicating some market incentives for higher-quality care, even for some ED admissions. Understanding these issues will help policymakers better define access to ED care and assist in directing quality improvement efforts. To our knowledge, our study is the most comprehensive nationwide characterization of patient travel for ED treatment to date.
大多数急诊科(ED)患者是自行前来就诊的,由于各种原因,他们可能不会选择最近的 ED。患者前往 ED 治疗的距离可能反映了患者获得医疗服务的途径和疾病的严重程度。在这项研究中,我们旨在检查患者前往的 ED 与患者家庭之间的旅行距离和旅行时间,并调查这些距离/时间如何因患者和医院特征而异。
我们随机抽取并收集了 2016 年 1 月至 3 月期间全国 50 家医院 ED 出院至社区(DTC)的 14812 名患者的数据。我们对患者和医院 ED 地址进行了地理编码和计算,并检查了患者家庭与他们就诊的 ED 之间的旅行距离/时间,使用混合效应回归模型调查了这些距离/时间如何因患者和医院特征而异。
患者前往 ED 的平均距离为 8.0(SD=10.9)英里,平均驾驶时间为 17.3(SD=18.0)分钟。患者为避免前往绩效较低的医院(p<0.01)和西部(p<0.05)和中西部(p<0.05)而前往 ED 的距离明显更远。患者前往农村地区的 ED 时,旅行距离更远。年轻患者比老年患者旅行距离更远。
了解患者愿意旅行的距离表明患者人群是否有足够的机会获得 ED 服务。通过表明患者为避免低绩效医院而旅行更远,我们提供了证据表明,DTC 患者可能在 ED 之间确实有一些选择,这表明存在一些对高质量护理的市场激励措施,即使是一些 ED 入院。了解这些问题将有助于决策者更好地定义 ED 护理的可及性,并有助于指导质量改进工作。据我们所知,我们的研究是迄今为止对 ED 治疗患者旅行最全面的全国性描述。