Trauma Research Unit, Department of Surgery, Erasmus MC, University Medical Center Rotterdam, P.O. Box 2040, 3000 CA, Rotterdam, The Netherlands.
Department of Anesthesiology, Erasmus University Medical Center Rotterdam, Rotterdam, The Netherlands.
Eur J Trauma Emerg Surg. 2022 Aug;48(4):3357-3372. doi: 10.1007/s00068-022-01941-y. Epub 2022 Mar 25.
Circulatory arrest after trauma is a life-threatening situation that mandates urgent action. The aims of this systematic review and meta-analysis on prehospital traumatic cardiac arrest (TCA) were to provide an updated pooled mortality rate for prehospital TCA, to investigate the impact of the time of patient inclusion and the type of prehospital trauma system on TCA mortality rates and neurological outcome, and to investigate which pre- and intra-arrest factors are prognostic for prehospital TCA mortality.
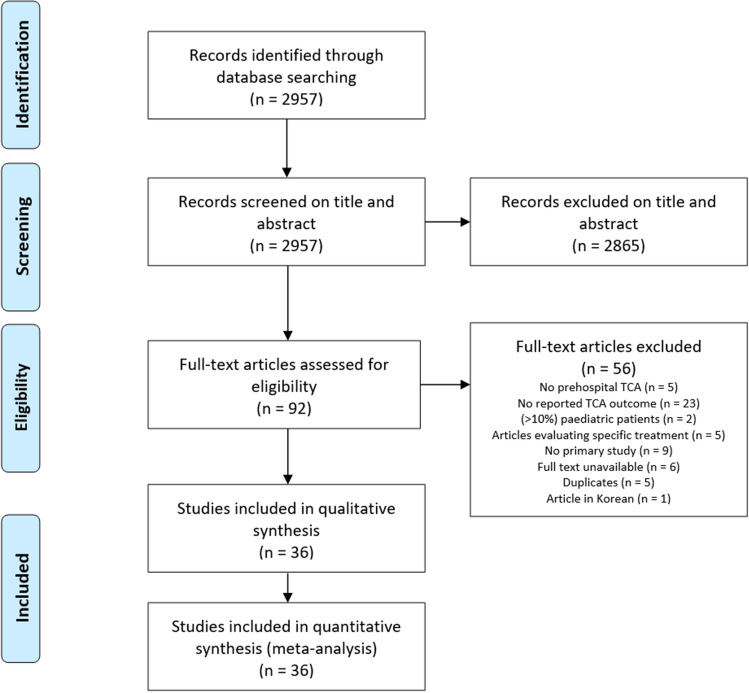
This review was conducted in accordance with the PRISMA and CHARMS guidelines. Databases were searched for primary studies published about prehospital TCA patients (1995-2020). Studies were divided into various EMS-system categories. Data were analyzed using MedCalc, Review Manager, Microsoft Excel, and Shinyapps Meta Power Calculator software.
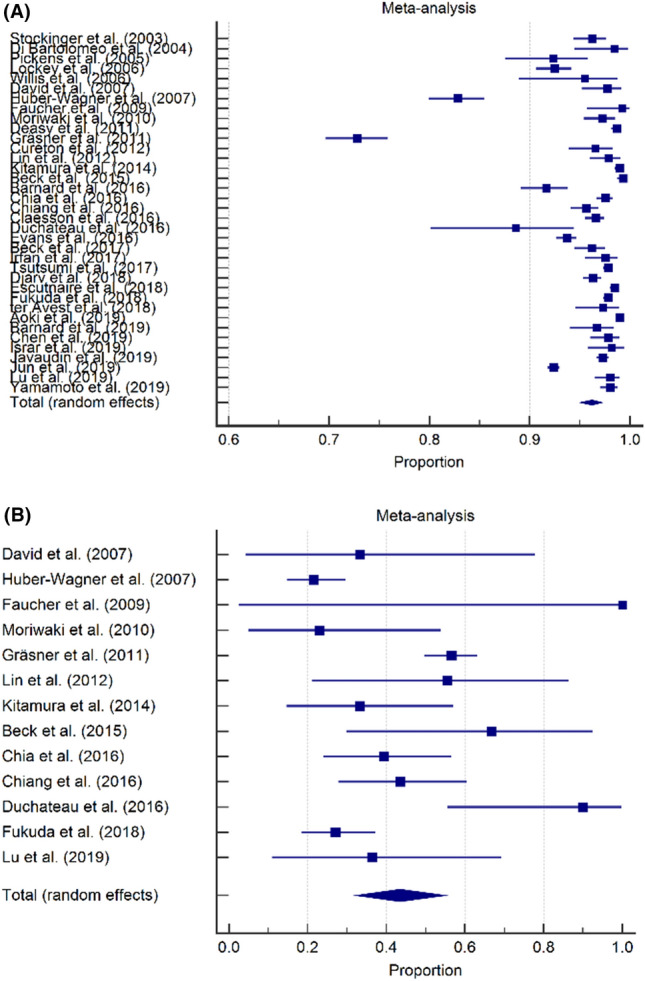
Thirty-six studies involving 51.722 patients were included. Overall mortality for TCA was 96.2% and a favorable neurological outcome was seen in 43.5% of the survivors. Mortality rates were 97.2% in studies including prehospital deaths and 92.3% in studies excluding prehospital deaths. Favorable neurological outcome rates were 35.8% in studies including prehospital deaths and 49.5% in studies excluding prehospital deaths. Mortality rates were 97.6% if no physician was available at the prehospital scene and 93.9% if a physician was available. Favorable neurological outcome rates were 57.0% if a physician was available on scene and 38.0% if no physician was available. Only non-shockable rhythm was associated with a higher mortality (RR 1.12, p = 0.06).
Approximately 1 in 20 patients with prehospital TCA will survive; about 40% of survivors have favorable neurological outcome.
创伤后心脏骤停是危及生命的紧急情况,需要立即采取行动。本系统评价和荟萃分析的目的是提供创伤性院前心脏骤停(TCA)的最新死亡率,研究患者纳入时间和院前创伤系统类型对 TCA 死亡率和神经结局的影响,并研究哪些院前和心搏骤停期间的因素与院前 TCA 死亡率相关。
本研究按照 PRISMA 和 CHARMS 指南进行。检索了自 1995 年至 2020 年发表的关于院前 TCA 患者的原始研究。研究分为各种 EMS 系统类别。使用 MedCalc、Review Manager、Microsoft Excel 和 Shinyapps Meta Power Calculator 软件分析数据。
共纳入 36 项研究,涉及 51722 例患者。TCA 的总体死亡率为 96.2%,幸存者中出现良好神经结局的比例为 43.5%。包括院前死亡的研究中死亡率为 97.2%,不包括院前死亡的研究中死亡率为 92.3%。包括院前死亡的研究中良好神经结局率为 35.8%,不包括院前死亡的研究中良好神经结局率为 49.5%。如果现场没有医生,死亡率为 97.6%,如果现场有医生,死亡率为 93.9%。如果现场有医生,良好的神经结局率为 57.0%,如果现场没有医生,良好的神经结局率为 38.0%。只有非可除颤节律与更高的死亡率相关(RR 1.12,p=0.06)。
大约每 20 例院前 TCA 患者中就有 1 例存活;约 40%的幸存者有良好的神经结局。