Department of Orthopedic Surgery, Ålesund Hospital, Møre and Romsdal Hospital Trust, Ålesund, Norway.
Kysthospitalet in Hagevik, Orthopedic Clinic, Haukeland University Hospital, Bergen, Norway.
JAMA Netw Open. 2022 Mar 1;5(3):e224291. doi: 10.1001/jamanetworkopen.2022.4291.
Operations for lumbar spinal stenosis is the most often performed surgical procedure in the adult lumbar spine. This study reports the clinical outcome of the 3 most commonly used minimally invasive posterior decompression techniques.
To compare the effectiveness of 3 minimally invasive posterior decompression techniques for lumbar spinal stenosis.
DESIGN, SETTING, AND PARTICIPANTS: This randomized clinical trial used a parallel group design and included patients with symptomatic and radiologically verified lumbar spinal stenosis without degenerative spondylolisthesis. Patients were enrolled between February 2014 and October 2018 at the orthopedic and neurosurgical departments of 16 Norwegian public hospitals. Statistical analysis was performed in the period from May to June 2021.
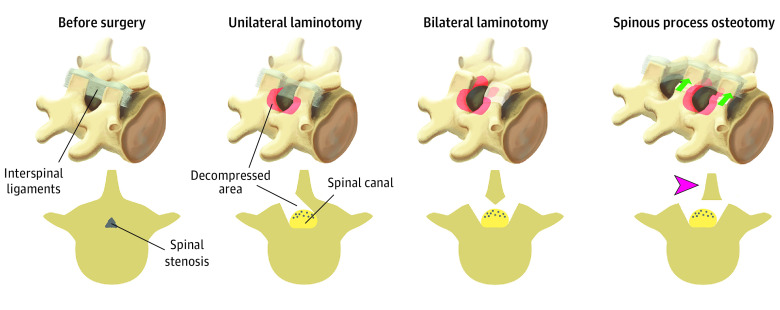
Patients were randomized to undergo 1 of the 3 minimally invasive posterior decompression techniques: unilateral laminotomy with crossover, bilateral laminotomy, and spinous process osteotomy.
Primary outcome was change in disability measured with Oswestry Disability Index (ODI; range 0-100), presented as mean change from baseline to 2-year follow-up and proportions of patients classified as success (>30% reduction in ODI). Secondary outcomes were mean change in quality of life, disease-specific symptom severity measured with Zurich Claudication Questionnaire (ZCQ), back pain and leg pain on a 10-point numeric rating score (NRS), patient perceived benefit of the surgical procedure, duration of the surgical procedure, blood loss, perioperative complications, number of reoperations, and length of hospital stay.
In total, 437 patients were included with a median (IQR) age of 68 (62-73) years and 230 men (53%). Of the included patients, 146 were randomized to unilateral laminotomy with crossover, 142 to bilateral laminotomy, and 149 to spinous process osteotomy. The unilateral laminotomy with crossover group had a mean change of -17.9 ODI points (95% CI, -20.8 to -14.9), the bilateral laminotomy group had a mean change of -19.7 ODI points (95% CI, -22.7 to -16.8), and the spinous process osteotomy group had a mean change of -19.9 ODI points (95% CI, -22.8 to -17.0). There were no significant differences in primary or secondary outcomes among the 3 surgical procedures, except a longer duration of the surgical procedure in the bilateral laminotomy group.
No differences in clinical outcomes or complication rates were found among the 3 minimally invasive posterior decompression techniques used to treat patients with lumbar spinal stenosis.
ClinicalTrials.gov Identifier: NCT02007083.
腰椎管狭窄症的手术是成人腰椎最常进行的手术。本研究报告了 3 种最常用的微创后路减压技术的临床结果。
比较 3 种微创后路减压技术治疗腰椎管狭窄症的效果。
设计、地点和参与者:这是一项随机临床试验,采用平行组设计,纳入了有症状和影像学证实的腰椎管狭窄症但无退行性脊椎滑脱的患者。患者于 2014 年 2 月至 2018 年 10 月在挪威 16 家公立医院的骨科和神经外科部门入组。统计分析于 2021 年 5 月至 6 月进行。
患者随机接受以下 3 种微创后路减压技术之一:单侧半椎板切除术交叉、双侧半椎板切除术和棘突截骨术。
主要结局为使用 Oswestry 功能障碍指数(ODI;范围 0-100)评估的残疾变化,表现为从基线到 2 年随访的平均变化以及分类为成功(ODI 降低>30%)的患者比例。次要结局为生活质量的平均变化、使用苏黎世跛行问卷(ZCQ)评估的疾病特异性症状严重程度、腰背疼痛和腿部疼痛的 10 分数字评分(NRS)、患者对手术的获益感知、手术持续时间、失血量、围手术期并发症、再次手术次数和住院时间。
共纳入 437 例患者,中位(IQR)年龄为 68(62-73)岁,230 例男性(53%)。纳入的患者中,146 例随机分配至单侧半椎板切除术交叉组,142 例至双侧半椎板切除术组,149 例至棘突截骨术组。单侧半椎板切除术交叉组 ODI 平均改善-17.9 分(95%CI,-20.8 至-14.9),双侧半椎板切除术组 ODI 平均改善-19.7 分(95%CI,-22.7 至-16.8),棘突截骨术组 ODI 平均改善-19.9 分(95%CI,-22.8 至-17.0)。3 种手术在主要或次要结局方面均无显著差异,除了双侧半椎板切除术组的手术持续时间较长。
治疗腰椎管狭窄症时,3 种微创后路减压技术的临床结果或并发症发生率无差异。
ClinicalTrials.gov 标识符:NCT02007083。