Gfrerer Lisa, Wong Frankie K, Hickle Kelli, Eberlin Kyle R, Valerio Ian L, Austen William G
Division of Plastic and Reconstructive Surgery, Massachusetts General Hospital, Harvard Medical School, Boston, Mass.
Plast Reconstr Surg Glob Open. 2022 Mar 25;10(3):e4201. doi: 10.1097/GOX.0000000000004201. eCollection 2022 Mar.
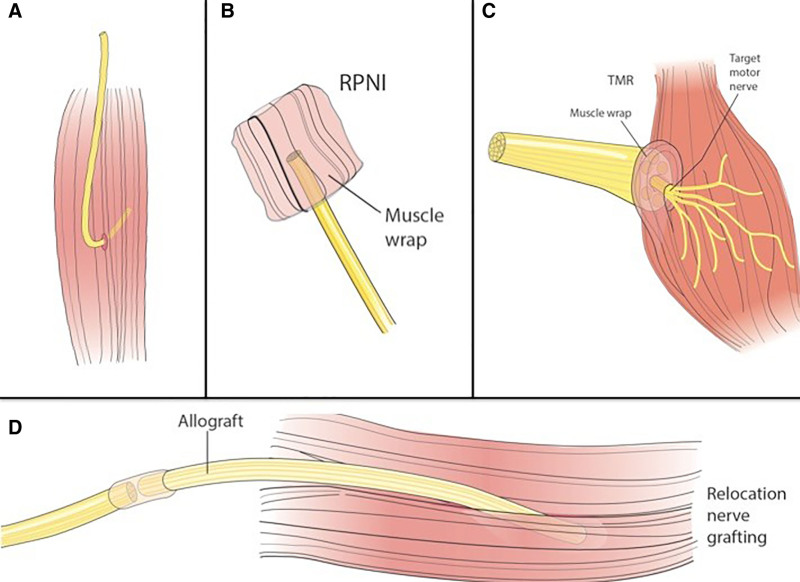
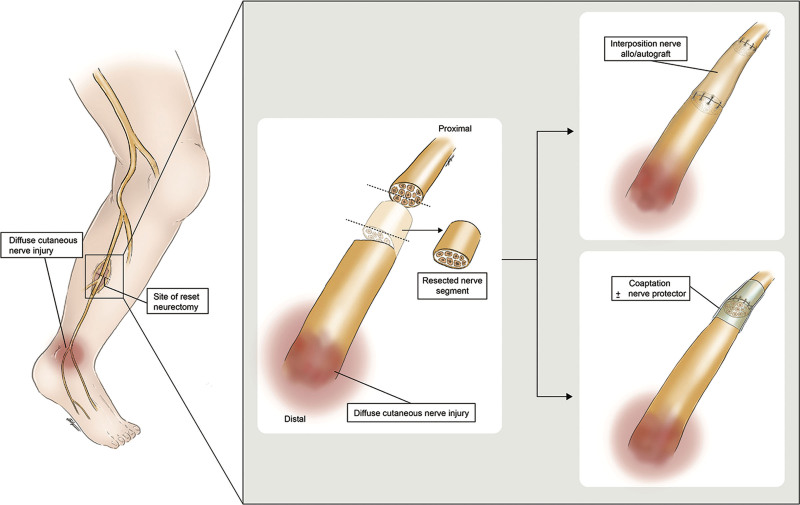
In the context of headache surgery, greater occipital nerve (GON) transection is performed when the nerve appears severely damaged, if symptoms are recurrent or persistent, and when neuromas are excised. Lesser occipital nerve (LON) excision is commonly performed during the primary decompression surgery. Advanced techniques to address the proximal nerve stump after nerve transection such as regenerative peripheral nerve interface (RPNI), targeted muscle reinnervation (TMR), relocation nerve grafting, and reset neurectomy have been shown to improve chronic pain and neuroma formation. These techniques have not been described in the head and neck region.
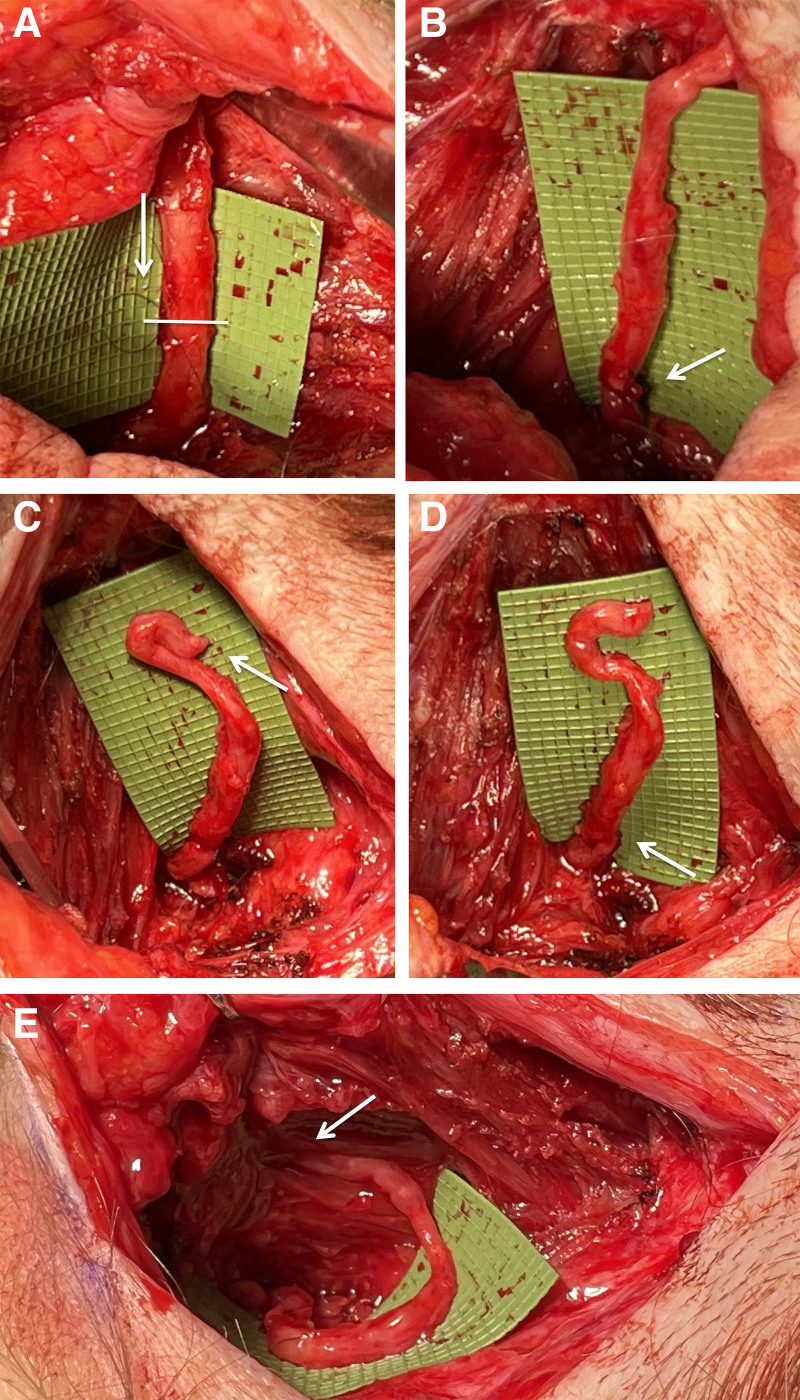
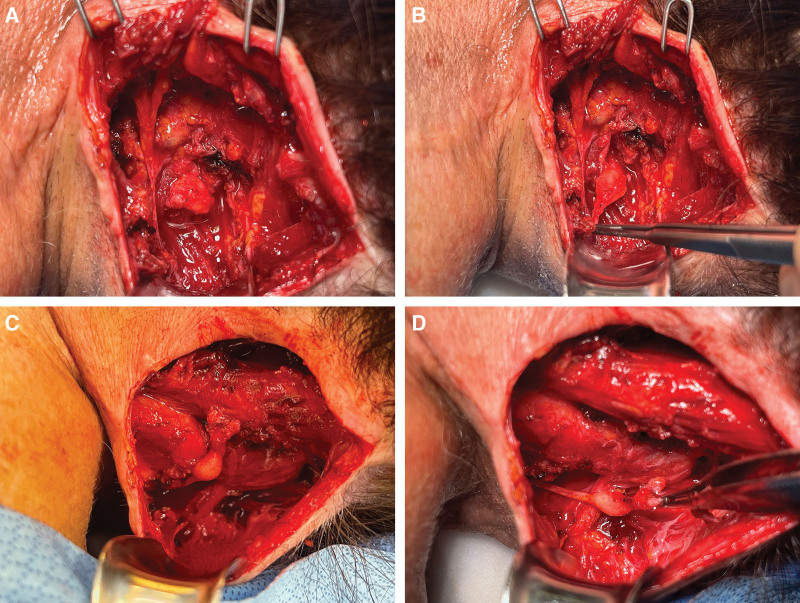
This article describes RPNI, TMR, and reset neurectomy with GON autograft relocation to prevent chronic pain and neuroma formation after GON/LON transection.
RPNI and TMR are feasible options in patients undergoing GON/LON transection. Further, relocation nerve grafting with GON autograft relocation is a method that is beneficial in patients with diffuse nerve injury requiring proximal nerve division.
Advanced nerve reconstruction techniques should be considered in headache surgery following GON/LON transection.
在头痛手术的背景下,当枕大神经(GON)严重受损、症状复发或持续以及切除神经瘤时,会进行枕大神经切断术。枕小神经(LON)切除通常在初次减压手术中进行。已证明,诸如再生周围神经接口(RPNI)、靶向肌肉再支配(TMR)、移位神经移植和重置神经切除术等处理神经切断术后近端神经残端的先进技术可改善慢性疼痛和神经瘤形成。这些技术尚未在头颈部区域得到描述。
本文描述了采用枕大神经自体移植移位的RPNI、TMR和重置神经切除术,以预防枕大神经/枕小神经切断术后的慢性疼痛和神经瘤形成。
RPNI和TMR对于接受枕大神经/枕小神经切断术的患者是可行的选择。此外,枕大神经自体移植移位的移位神经移植是一种对需要近端神经切断的弥漫性神经损伤患者有益的方法。
在枕大神经/枕小神经切断术后的头痛手术中应考虑采用先进的神经重建技术。