Nuffield Department of Primary Care Health Sciences, University of Oxford, Oxford, UK
Chipping Surgery, Wotton-under-Edge, UK.
BMJ Qual Saf. 2022 Jul;31(7):541-554. doi: 10.1136/bmjqs-2021-014529. Epub 2022 Mar 30.
Safety-netting has become best practice when dealing with diagnostic uncertainty in primary care. Its use, however, is highly varied and a lack of evidence-based guidance on its communication could be harming its effectiveness and putting patient safety at risk.
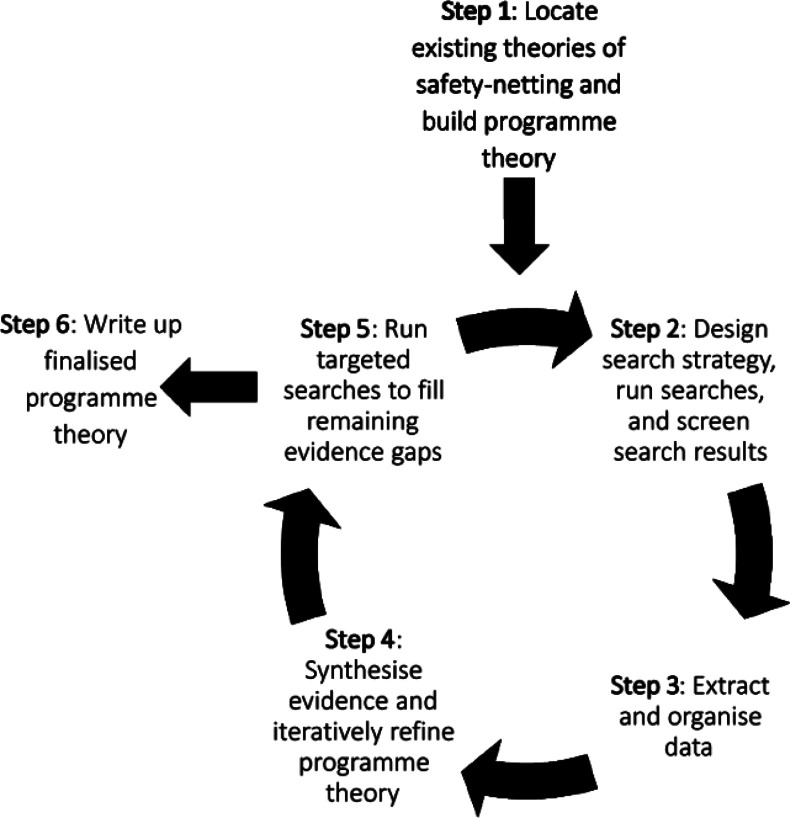
To use a realist review method to produce a programme theory of safety-netting, that is, advice and support provided to patients when diagnosis or prognosis is uncertain, in primary care.
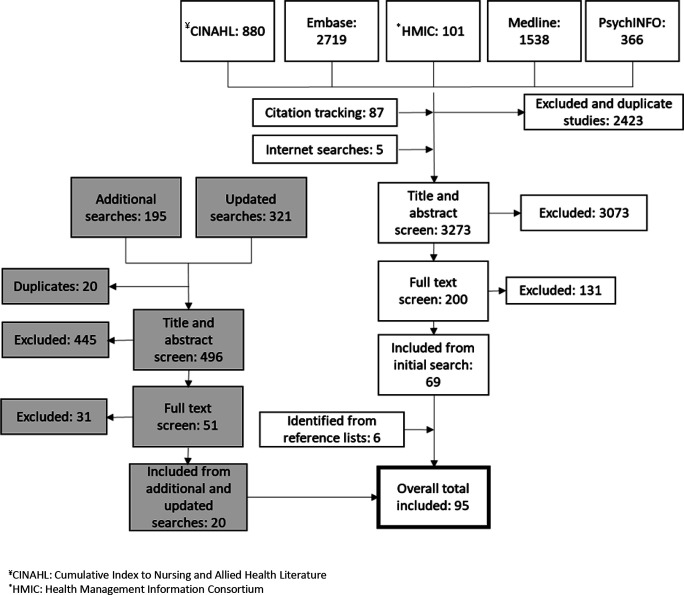
Five electronic databases, web searches, and grey literature were searched for studies assessing outcomes related to understanding and communicating safety-netting advice or risk communication, or the ability of patients to self-care and re-consult when appropriate. Characteristics of included documents were extracted into an Excel spreadsheet, and full texts uploaded into NVivo and coded. A random 10% sample was independently double -extracted and coded. Coded data wasere synthesised and itstheir ability to contribute an explanation for the contexts, mechanisms, or outcomes of effective safety-netting communication considered. Draft context, mechanism and outcome configurations (CMOCs) were written by the authors and reviewed by an expert panel of primary care professionals and patient representatives.
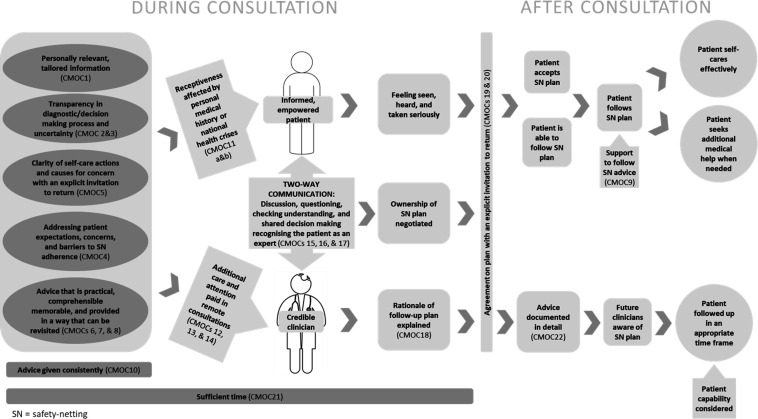
95 documents contributed to our CMOCs and programme theory. Effective safety-netting advice should be tailored to the patient and provide practical information for self-care and reconsultation. The importance of ensuring understanding and agreement with advice was highlighted, as was consideration of factors such as previous experiences with healthcare, the patient's personal circumstances and the consultation setting. Safety-netting advice should be documented in sufficient detail to facilitate continuity of care.
We present 15 recommendations to enhance communication of safety-netting advice and map these onto established consultation models. Effective safety-netting communication relies on understanding the information needs of the patient, barriers to acceptance and explanation of the reasons why the advice is being given. Reduced continuity of care, increasing multimorbidity and remote consultations represent threats to safety-netting communication.
在初级保健中处理诊断不确定性时,安全网已成为最佳实践。然而,其使用方式差异很大,缺乏循证指导可能会降低其有效性并使患者安全面临风险。
使用真实主义审查方法生成初级保健中安全网(即在诊断或预后不确定时为患者提供的建议和支持)的方案理论。
检索了五个电子数据库、网络搜索和灰色文献,以评估与理解和沟通安全网建议或风险沟通相关的结果,或患者在适当情况下自我护理和重新咨询的能力的研究。将纳入文献的特征提取到 Excel 电子表格中,并将全文上传到 NVivo 并进行编码。对随机抽取的 10%的样本进行独立的双提取和编码。对编码数据进行综合分析,并考虑其对有效安全网沟通的背景、机制或结果的解释能力。作者编写了草稿背景、机制和结果配置(CMOC),并由初级保健专业人员和患者代表的专家小组进行了审查。
95 篇文献为我们的 CMOC 和方案理论做出了贡献。有效的安全网建议应根据患者情况量身定制,并提供自我护理和重新咨询的实用信息。确保理解和同意建议的重要性得到了强调,同时还考虑了之前的医疗保健经历、患者的个人情况和咨询环境等因素。安全网建议应详细记录,以方便医疗服务的连续性。
我们提出了 15 条增强安全网建议沟通的建议,并将这些建议映射到现有的咨询模型上。有效的安全网沟通依赖于了解患者的信息需求、接受障碍以及解释提供建议的原因。医疗服务连续性的降低、不断增加的多病共存和远程咨询对安全网沟通构成了威胁。