Division of Cardiology, Columbia University Irving Medical Center/New York-Presbyterian Hospital, New York, New York, USA; Richard A. and Susan F. Smith Center for Outcomes Research, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, Massachusetts, USA.
Division of Cardiology, New York University Langone Health & Grossman School of Medicine, New York, New York, USA.
J Am Coll Cardiol. 2022 Apr 5;79(13):1223-1235. doi: 10.1016/j.jacc.2022.01.037.
Mortality rates for patients presenting with acute myocardial infarction (AMI) and cardiogenic shock (CS) remain high despite advances in revascularization strategies and mechanical circulatory support (MCS) devices.
This study sought to elucidate the association between comorbid lower extremity peripheral artery disease (PAD) and outcomes in CS and AMI.
PAD status was defined in Medicare beneficiaries hospitalized with CS and AMI from October 1, 2015 to June 30, 2018. Primary outcomes ascertained through December 31, 2018 included in- and out-of-hospital mortality. Secondary outcomes included bleeding, amputation, stroke, and lower extremity revascularization. Multivariable regression models with adjustment for confounders were used to estimate risk. Subgroup analyses included patients treated with MCS and those who underwent coronary revascularization.
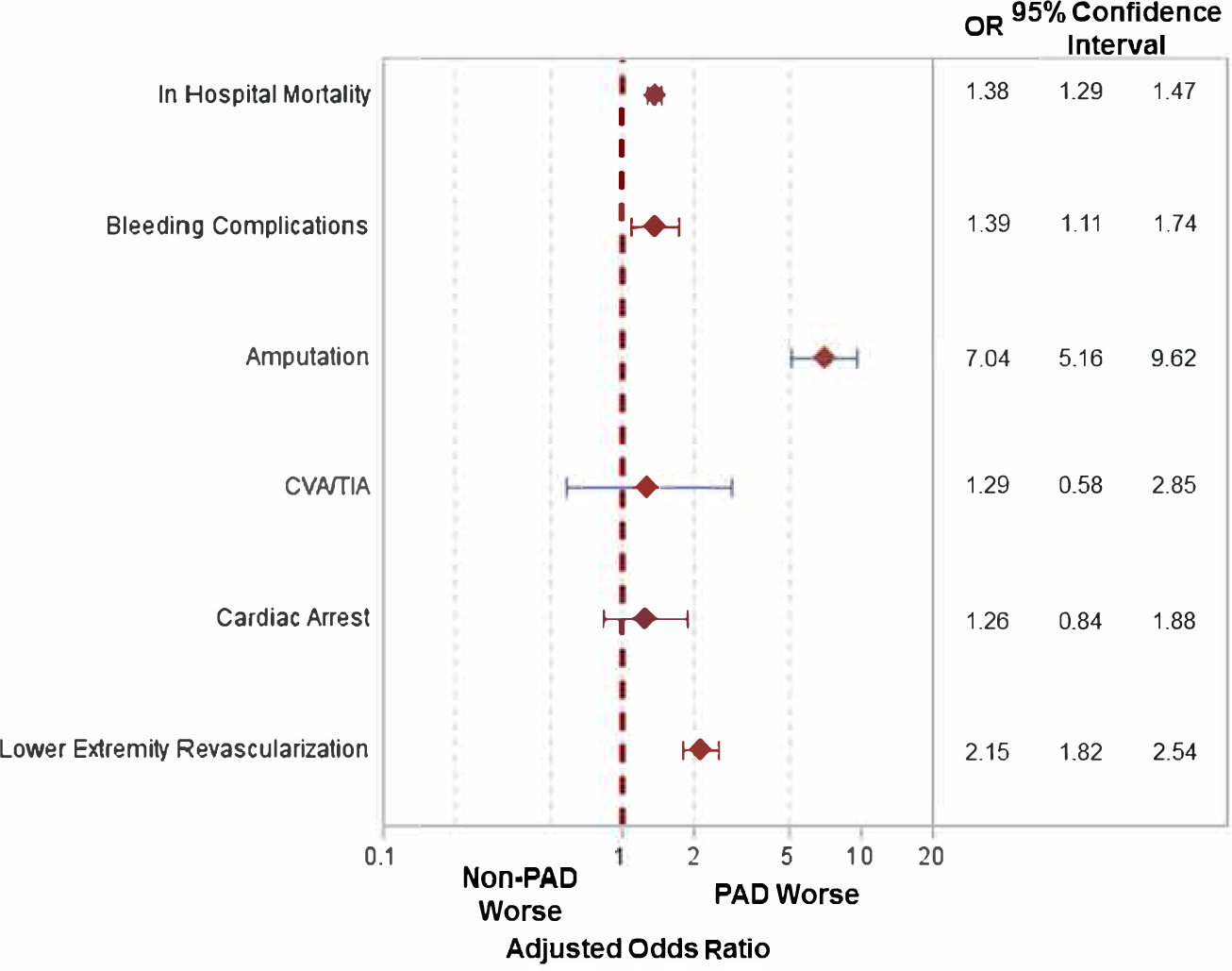
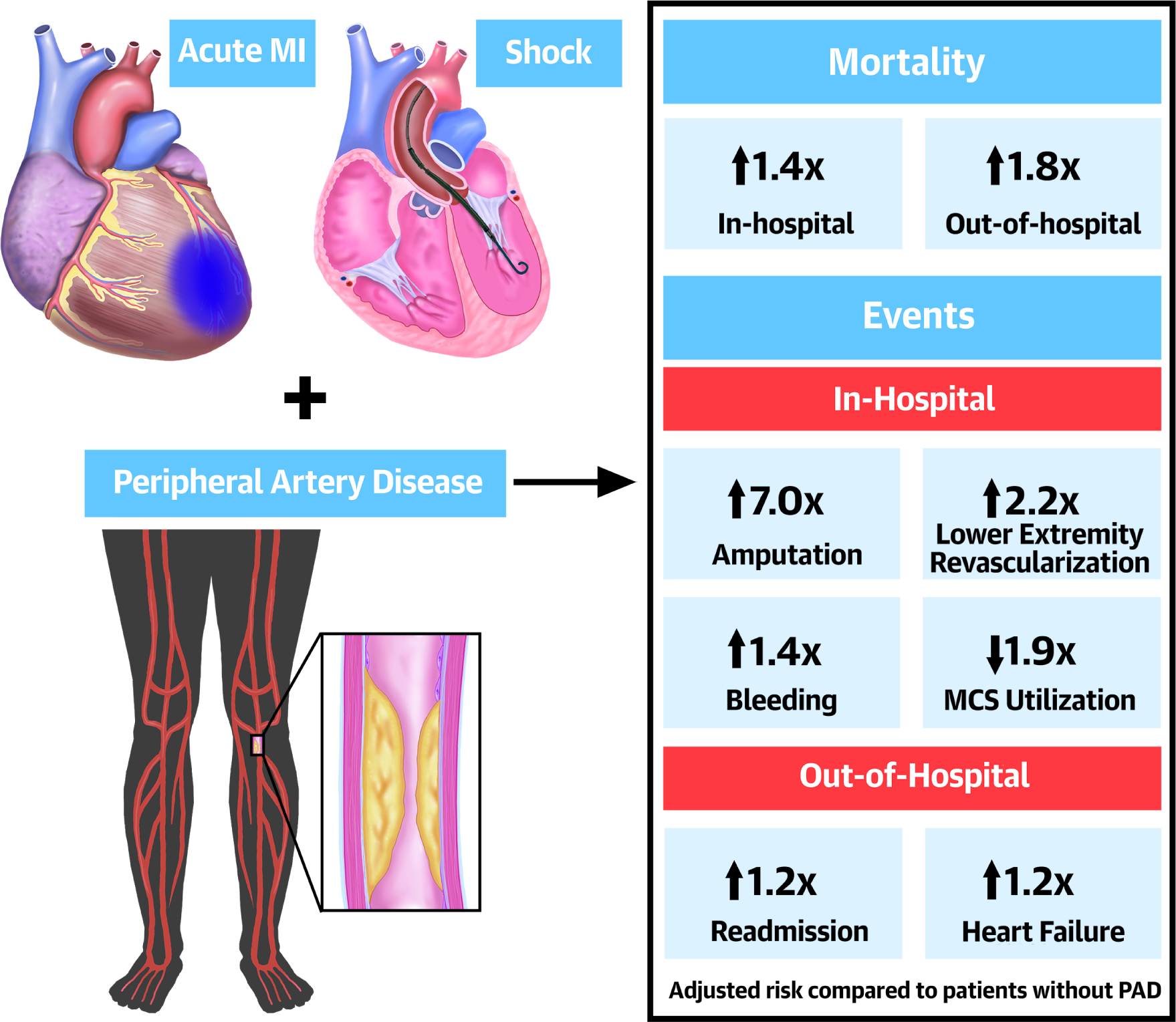
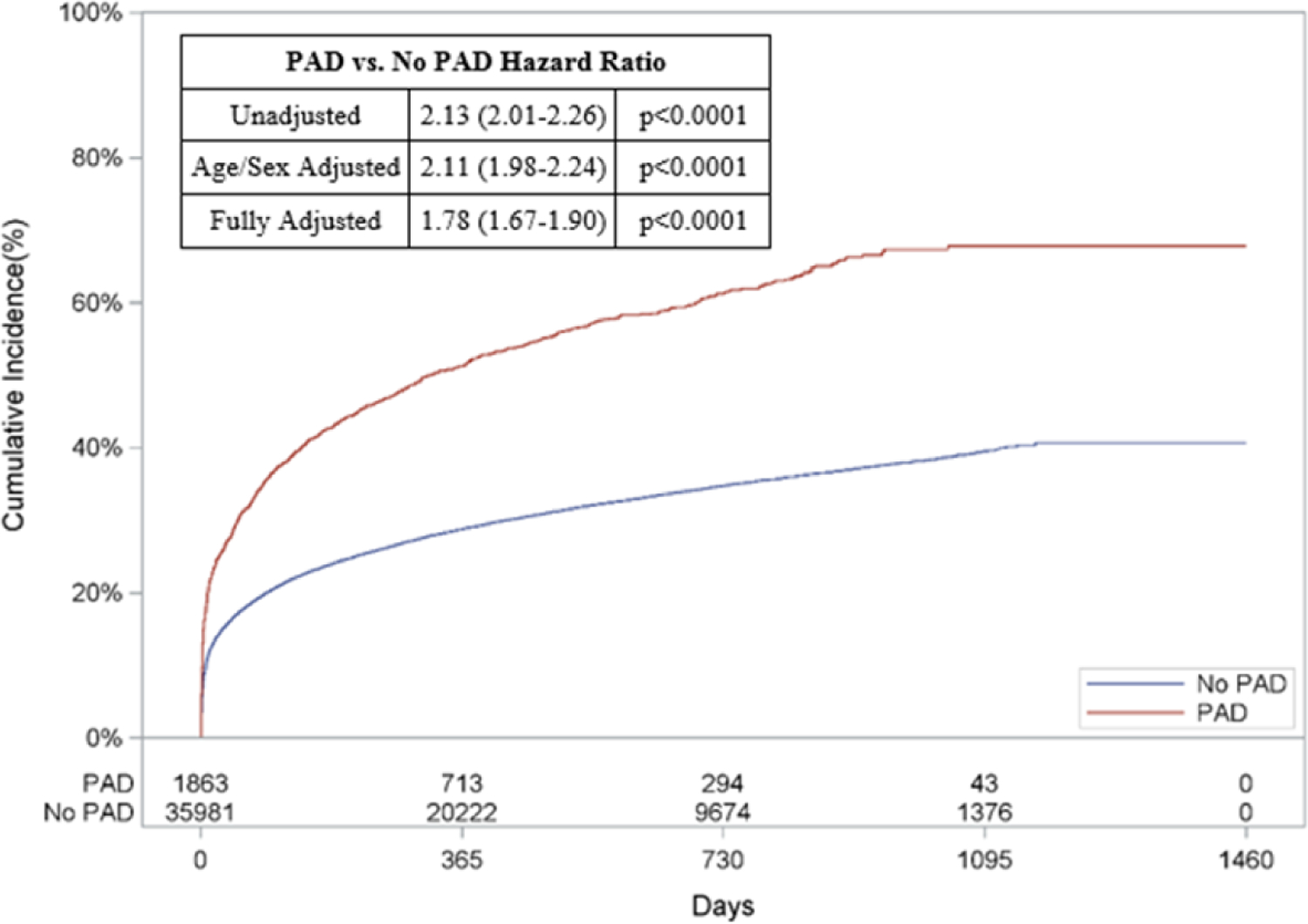
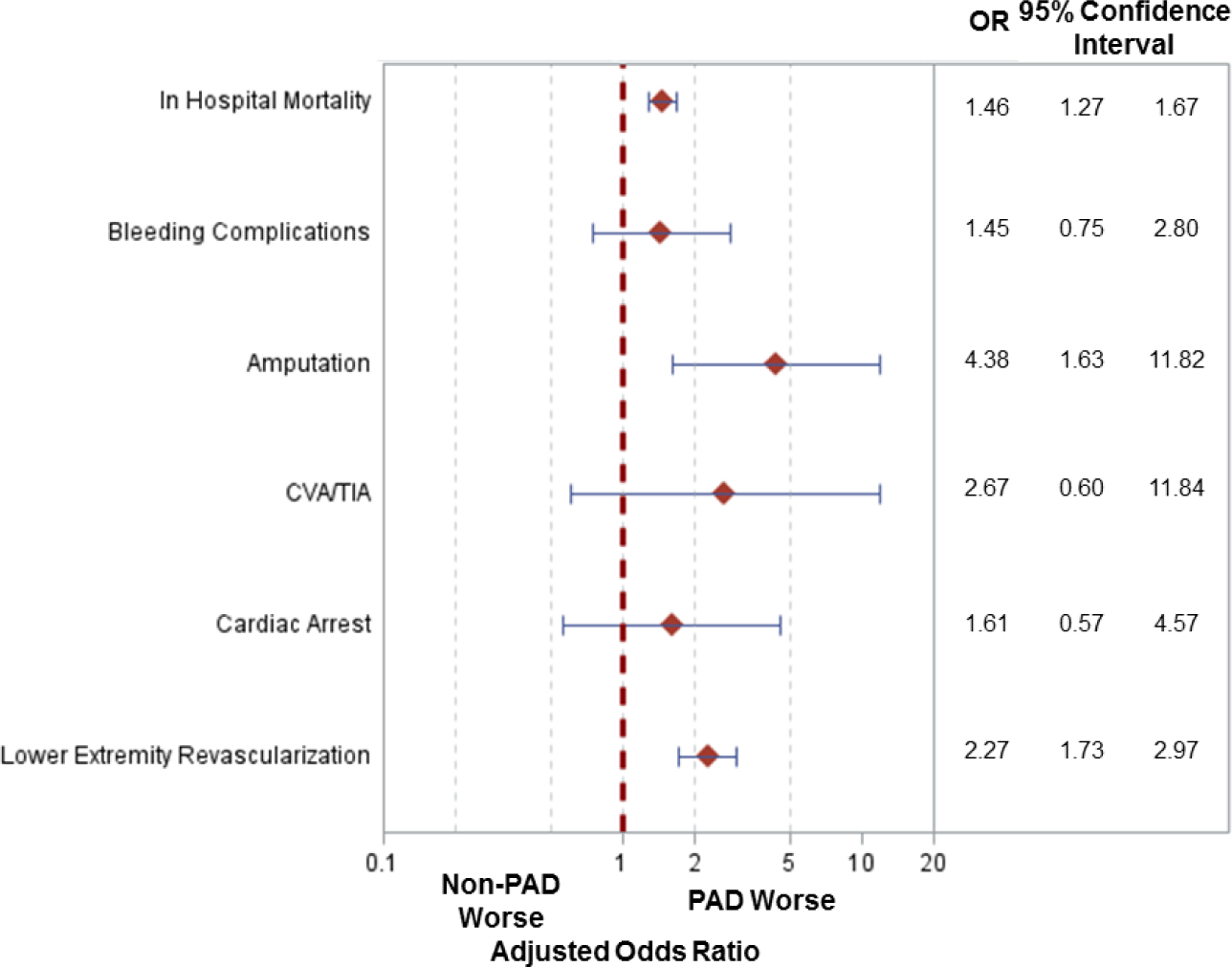
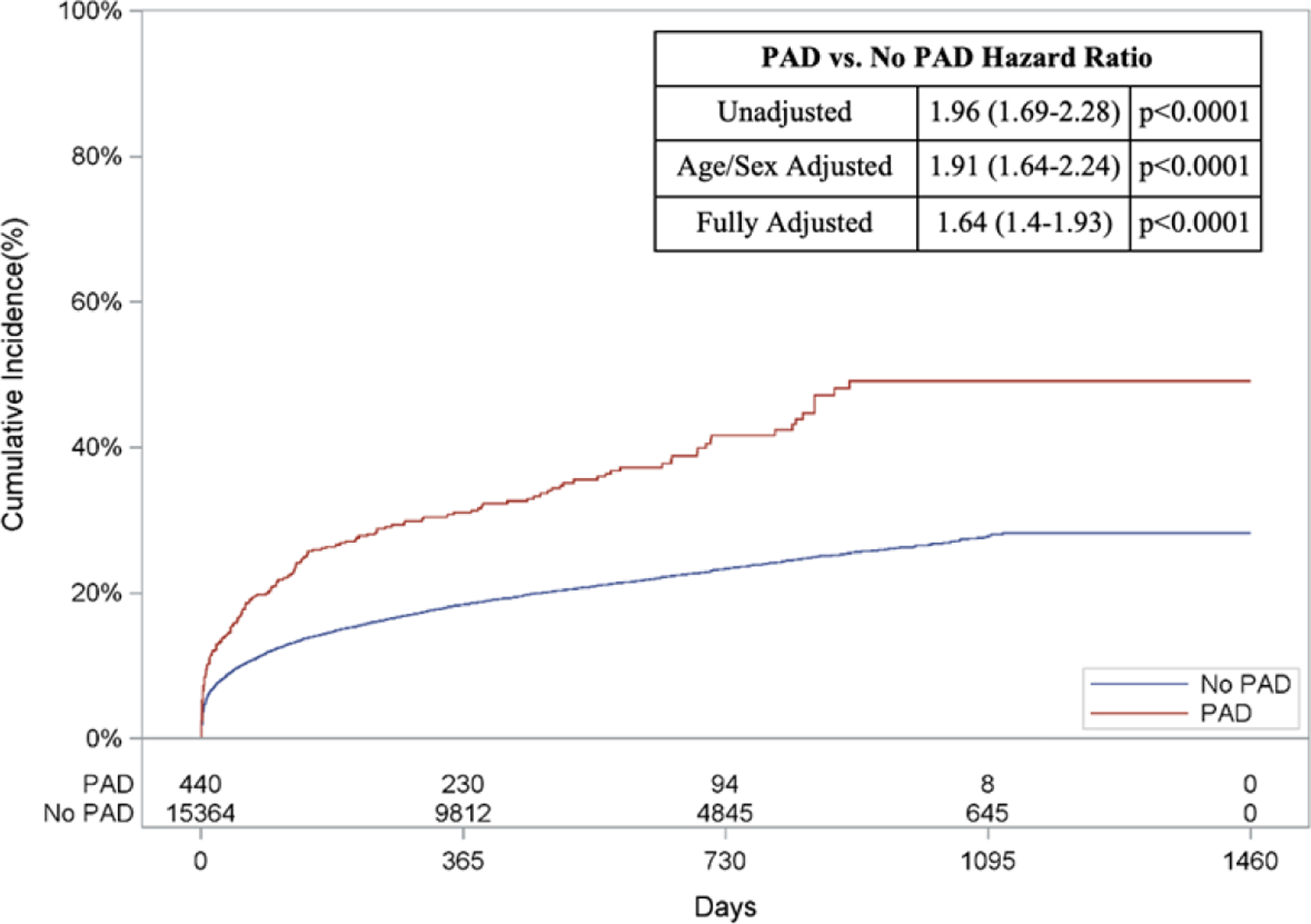
Among 71,690 patients, 5.9% (N = 4,259) had PAD. Mean age was 77.8 ± 7.9 years, 58.7% were male, and 84.3% were White. Cumulative in-hospital mortality was 47.2%, with greater risk among those with PAD (56.3% vs 46.6% without PAD; adjusted OR: 1.50; 95% CI: 1.40-1.59). PAD patients also had greater risk of in-hospital amputation (1.6% vs 0.2%; adjusted OR: 7.0; 95% CI: 5.26-9.37) and out-of-hospital mortality (67.9% vs 40.7%; adjusted HR: 1.78; 95% CI: 1.67-1.90). MCS was less frequently utilized in PAD patients (21.5% vs 38.6% without PAD; P < 0.001) and was associated with higher mortality, need for lower extremity revascularization, and amputation risk. Findings were consistent in patients who underwent coronary revascularization.
Among patients presenting with AMI and CS, PAD was associated with worse limb outcomes and survival. In addition to lower MCS utilization rates, those with PAD who received MCS had increased mortality, lower extremity revascularization, and amputation rates.
尽管在血运重建策略和机械循环支持(MCS)设备方面取得了进展,患有急性心肌梗死(AMI)和心源性休克(CS)的患者的死亡率仍然很高。
本研究旨在阐明合并下肢外周动脉疾病(PAD)与 CS 和 AMI 患者预后之间的关系。
2015 年 10 月 1 日至 2018 年 6 月 30 日,在 Medicare 受益人因 CS 和 AMI 住院期间确定 PAD 状态。通过 2018 年 12 月 31 日确定的主要预后包括院内和院外死亡率。次要预后包括出血、截肢、卒中和下肢血运重建。使用多变量回归模型调整混杂因素来估计风险。亚组分析包括接受 MCS 治疗和接受冠状动脉血运重建的患者。
在 71690 名患者中,5.9%(N=4259)患有 PAD。平均年龄为 77.8±7.9 岁,58.7%为男性,84.3%为白人。住院期间的累积死亡率为 47.2%,PAD 患者的风险更高(56.3% vs 46.6%无 PAD;调整后的 OR:1.50;95%CI:1.40-1.59)。PAD 患者也有更高的住院期间截肢风险(1.6% vs 0.2%;调整后的 OR:7.0;95%CI:5.26-9.37)和院外死亡率(67.9% vs 40.7%;调整后的 HR:1.78;95%CI:1.67-1.90)。PAD 患者的 MCS 使用率较低(21.5% vs 38.6%无 PAD;P<0.001),且与死亡率较高、需要下肢血运重建和截肢风险相关。在接受冠状动脉血运重建的患者中,发现结果一致。
在患有 AMI 和 CS 的患者中,PAD 与较差的肢体预后和生存相关。除了较低的 MCS 使用率外,接受 MCS 的 PAD 患者死亡率更高,需要下肢血运重建和截肢率更高。