Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA; Emory Center for Heart Disease Prevention, Emory University School of Medicine, Atlanta, Georgia, USA.
Johns Hopkins Ciccarone Center for the Prevention of Cardiovascular Disease, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA.
JACC Cardiovasc Imaging. 2022 Jul;15(7):1259-1270. doi: 10.1016/j.jcmg.2022.02.011. Epub 2022 Mar 21.
Coronary artery calcium (CAC) is a marker of plaque burden. Whether CAC improves risk stratification for incident sudden cardiac death (SCD) beyond atherosclerotic cardiovascular disease (ASCVD) risk factors is unknown.
SCD is a common initial manifestation of coronary heart disease (CHD); however, SCD risk prediction remains elusive.
The authors studied 66,636 primary prevention patients from the CAC Consortium. Multivariable competing risks regression and C-statistics were used to assess the association between CAC and SCD, adjusting for demographics and traditional risk factors.
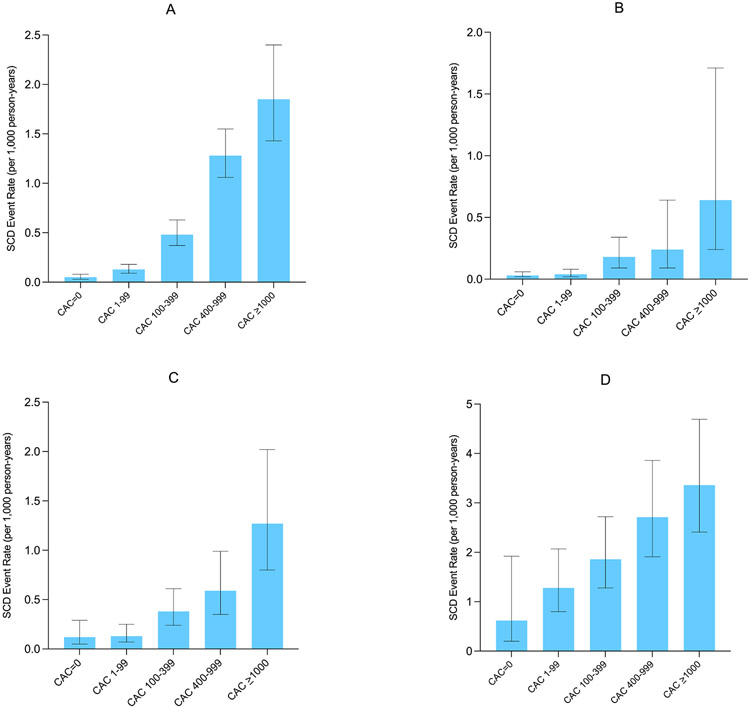
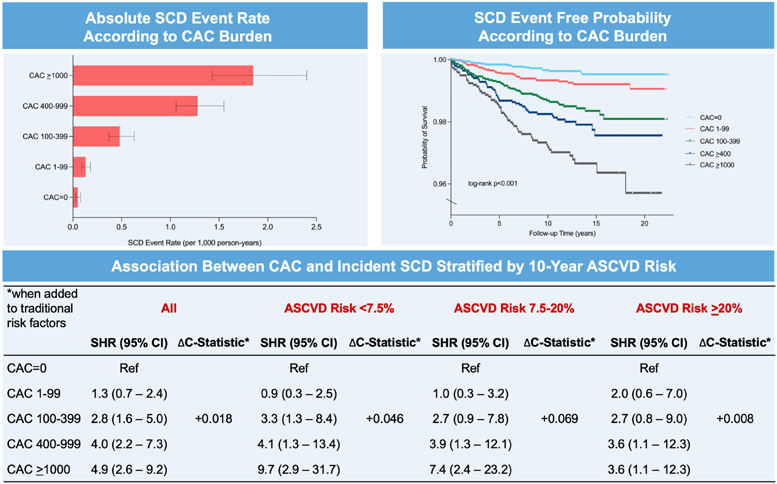
The mean age was 54.4 years, 33% were women, 11% were of non-White ethnicity, and 55% had CAC >0. A total of 211 SCD events (0.3%) were observed during a median follow-up of 10.6 years, 91% occurring among those with baseline CAC >0. Compared with CAC = 0, there was a stepwise higher risk (P trend < 0.001) in SCD for CAC 100 to 399 (subdistribution hazard ratio [SHR]: 2.8; 95% CI: 1.6-5.0), CAC 400 to 999 (SHR: 4.0; 95% CI: 2.2-7.3), and CAC >1,000 (SHR: 4.9; 95% CI: 2.6-9.9). CAC provided incremental improvements in the C-statistic for the prediction of SCD among individuals with a 10-year risk <7.5% (ΔC-statistic = +0.046; P = 0.02) and 7.5% to 20% (ΔC-statistic = +0.069; P = 0.003), which were larger when compared with persons with a 10-year risk >20% (ΔC-statistic = +0.01; P = 0.54).
Higher CAC burden strongly associates with incident SCD beyond traditional risk factors, particularly among primary prevention patients with low-intermediate risk. SCD risk stratification can be useful in the early stages of CHD through the measurement of CAC, identifying patients most likely to benefit from further downstream testing.
冠状动脉钙(CAC)是斑块负担的标志物。CAC 是否可以改善突发心脏性死亡(SCD)的风险分层,超过动脉粥样硬化性心血管疾病(ASCVD)的危险因素尚不清楚。
SCD 是冠心病(CHD)的常见首发表现;然而,SCD 风险预测仍难以捉摸。
作者研究了 CAC 联盟的 66636 名一级预防患者。采用多变量竞争风险回归和 C 统计量评估 CAC 与 SCD 之间的关联,调整了人口统计学和传统危险因素。
平均年龄为 54.4 岁,33%为女性,11%为非白人,55%的 CAC>0。在中位随访 10.6 年期间,共观察到 211 例 SCD 事件(0.3%),91%发生在基线 CAC>0 的患者中。与 CAC=0 相比,CAC 100 至 399(亚分布危险比 [SHR]:2.8;95%置信区间 [CI]:1.6-5.0)、CAC 400 至 999(SHR:4.0;95%CI:2.2-7.3)和 CAC>1000(SHR:4.9;95%CI:2.6-9.9)的 SCD 风险呈递增趋势(P 趋势<0.001)。在 10 年风险<7.5%的个体中(ΔC 统计量=+0.046;P=0.02)和 7.5%至 20%的个体中(ΔC 统计量=+0.069;P=0.003),CAC 对 SCD 预测的 C 统计量有增量改善,而在 10 年风险>20%的个体中(ΔC 统计量=+0.01;P=0.54),这种改善较小。
较高的 CAC 负担与传统危险因素以外的事件性 SCD 强烈相关,尤其是在低-中危的一级预防患者中。通过 CAC 测量,SCD 风险分层可用于 CHD 的早期阶段,识别最有可能从进一步下游检查中获益的患者。