Butler Liam, Ivanov Alexander, Celik Turgay, Karabayir Ibrahim, Chinthala Lokesh, Hudson Melissa M, Ness Kiri K, Mulrooney Daniel A, Dixon Stephanie B, Tootooni Mohammad S, Doerr Adam J, Jaeger Byron C, Davis Robert L, McManus David D, Herrington David, Akbilgic Oguz
Cardiovascular Section, Department of Internal Medicine, Wake Forest University School of Medicine, Winston-Salem, North Carolina.
Center for Biomedical Informatics, University of Tennessee Health Sciences Center, Memphis, Tennessee.
Cardiovasc Digit Health J. 2024 Apr 5;5(3):115-121. doi: 10.1016/j.cvdhj.2024.03.007. eCollection 2024 Jun.
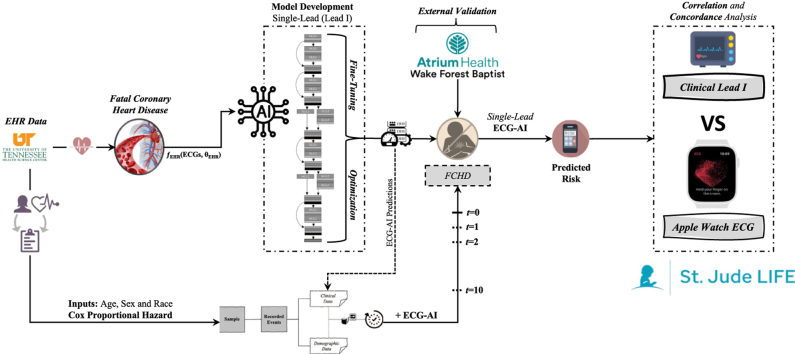
Fatal coronary heart disease (FCHD) is often described as sudden cardiac death (affects >4 million people/year), where coronary artery disease is the only identified condition. Electrocardiographic artificial intelligence (ECG-AI) models for FCHD risk prediction using ECG data from wearable devices could enable wider screening/monitoring efforts.
To develop a single-lead ECG-based deep learning model for FCHD risk prediction and assess concordance between clinical and Apple Watch ECGs.
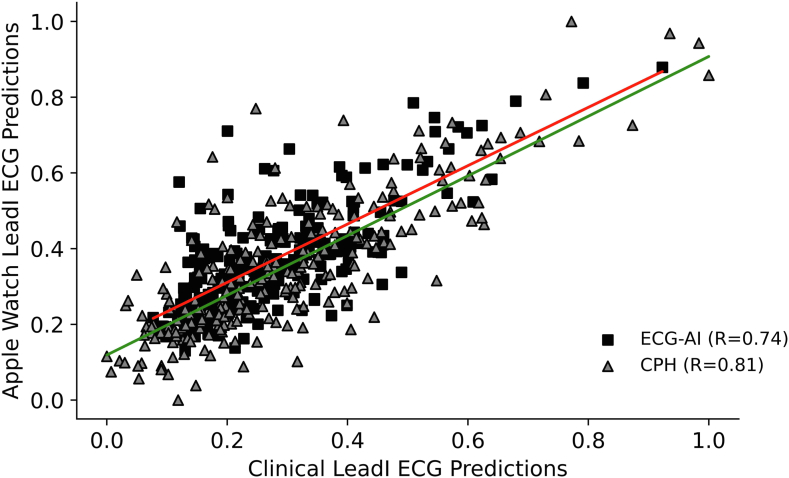
An FCHD single-lead ("lead I" from 12-lead ECGs) ECG-AI model was developed using 167,662 ECGs (50,132 patients) from the University of Tennessee Health Sciences Center. Eighty percent of the data (5-fold cross-validation) was used for training and 20% as a holdout. Cox proportional hazards (CPH) models incorporating ECG-AI predictions with age, sex, and race were also developed. The models were tested on paired clinical single-lead and Apple Watch ECGs from 243 St. Jude Lifetime Cohort Study participants. The correlation and concordance of the predictions were assessed using Pearson correlation (R), Spearman correlation (ρ), and Cohen's kappa.
The ECG-AI and CPH models resulted in AUC = 0.76 and 0.79, respectively, on the 20% holdout and AUC = 0.85 and 0.87 on the Atrium Health Wake Forest Baptist external validation data. There was moderate-strong positive correlation between predictions (R = 0.74, ρ = 0.67, and κ = 0.58) when tested on the 243 paired ECGs. The clinical (lead I) and Apple Watch predictions led to the same low/high-risk FCHD classification for 99% of the participants. CPH prediction correlation resulted in an R = 0.81, ρ = 0.76, and κ = 0.78.
Risk of FCHD can be predicted from single-lead ECGs obtained from wearable devices and are statistically concordant with lead I of a 12-lead ECG.
致命性冠心病(FCHD)通常被描述为心源性猝死(每年影响超过400万人),其中冠状动脉疾病是唯一已确定的病症。利用可穿戴设备的心电图数据进行FCHD风险预测的心电图人工智能(ECG-AI)模型能够推动更广泛的筛查/监测工作。
开发一种基于单导联心电图的深度学习模型用于FCHD风险预测,并评估临床心电图与苹果手表心电图之间的一致性。
使用田纳西大学健康科学中心的167,662份心电图(50,132名患者)开发了一个FCHD单导联(来自12导联心电图的“导联I”)ECG-AI模型。80%的数据(5折交叉验证)用于训练,20%作为保留数据。还开发了将ECG-AI预测与年龄、性别和种族相结合的Cox比例风险(CPH)模型。这些模型在来自243名圣裘德终身队列研究参与者的配对临床单导联和苹果手表心电图上进行了测试。使用Pearson相关性(R)、Spearman相关性(ρ)和Cohen's kappa评估预测的相关性和一致性。
在20%的保留数据上,ECG-AI模型和CPH模型的AUC分别为0.76和0.79,在阿特里姆健康韦克福里斯特浸礼会外部验证数据上的AUC分别为0.85和0.87。在对243对心电图进行测试时,预测之间存在中度至强的正相关性(R = 0.74,ρ = 0.67,κ = 0.58)。临床(导联I)和苹果手表的预测对99%的参与者得出了相同的低/高风险FCHD分类。CPH预测相关性得出R = 0.81,ρ = 0.76,κ = 0.78。
可从可穿戴设备获得的单导联心电图预测FCHD风险,并且在统计学上与12导联心电图的导联I一致。