Kortz Teresa B, Nielsen Katie R, Mediratta Rishi P, Reeves Hailey, O'Brien Nicole F, Lee Jan Hau, Attebery Jonah E, Bhutta Emaan G, Biewen Carter, Coronado Munoz Alvaro, deAlmeida Mary L, Fonseca Yudy, Hooli Shubhada, Johnson Hunter, Kissoon Niranjan, Leimanis-Laurens Mara L, McCarthy Amanda M, Pineda Carol, Remy Kenneth E, Sanders Sara C, Takwoingi Yemisi, Wiens Matthew O, Bhutta Adnan T
Division of Critical Care, Department of Pediatrics, University of California, San Francisco, San Francisco, CA, United States.
Institute for Global Health Sciences, University of California, San Francisco, San Francisco, CA, United States.
Front Pediatr. 2022 Mar 16;10:756643. doi: 10.3389/fped.2022.756643. eCollection 2022.
The majority of childhood deaths occur in low- and middle-income countries (LMICs). Many of these deaths are avoidable with basic critical care interventions. Quantifying the burden of pediatric critical illness in LMICs is essential for targeting interventions to reduce childhood mortality.
To determine the burden of hospitalization and mortality associated with acute pediatric critical illness in LMICs through a systematic review and meta-analysis of the literature.
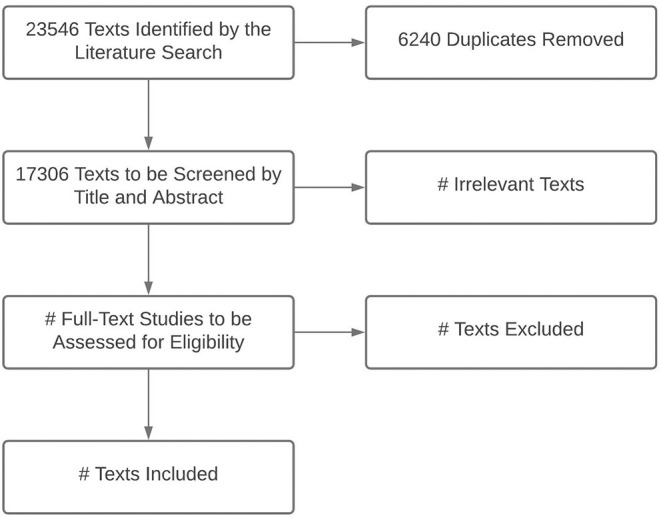
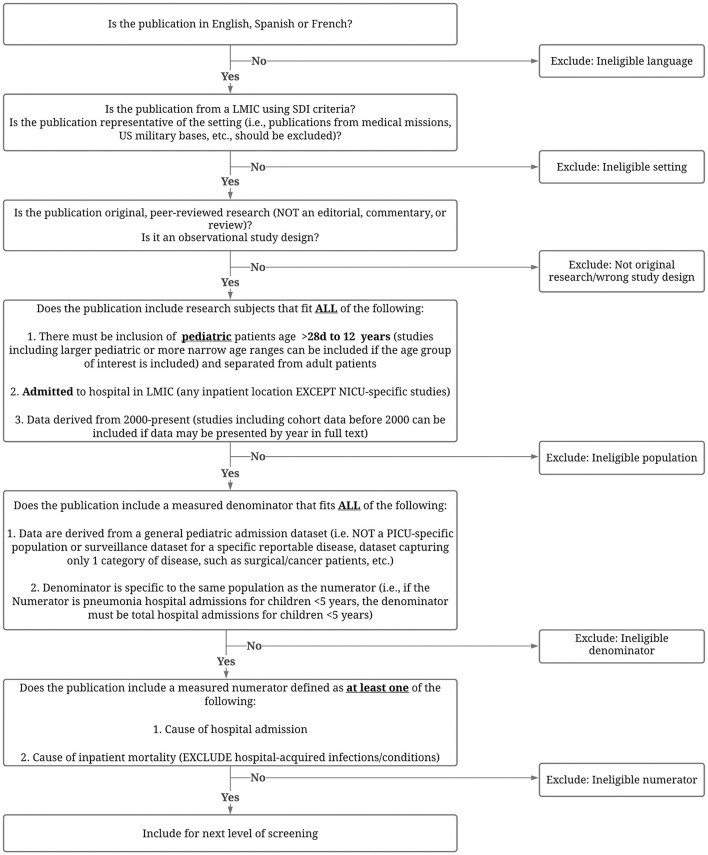
We will identify eligible studies by searching MEDLINE, EMBASE, CINAHL, and LILACS using MeSH terms and keywords. Results will be limited to infants or children (ages >28 days to 12 years) hospitalized in LMICs and publications in English, Spanish, or French. Publications with non-original data (e.g., comments, editorials, letters, notes, conference materials) will be excluded.
We will include observational studies published since January 1, 2005, that meet all eligibility criteria and for which a full text can be located.
Data extraction will include information related to study characteristics, hospital characteristics, underlying population characteristics, patient population characteristics, and outcomes.
We will extract and report data on study, hospital, and patient characteristics; outcomes; and risk of bias. We will report the causes of admission and mortality by region, country income level, and age. We will report or calculate the case fatality rate (CFR) for each diagnosis when data allow.
By understanding the burden of pediatric critical illness in LMICs, we can advocate for resources and inform resource allocation and investment decisions to improve the management and outcomes of children with acute pediatric critical illness in LMICs.
大多数儿童死亡发生在低收入和中等收入国家(LMICs)。通过基本的重症监护干预措施,其中许多死亡是可以避免的。量化低收入和中等收入国家儿科危重症的负担对于针对性干预以降低儿童死亡率至关重要。
通过对文献的系统评价和荟萃分析,确定低收入和中等收入国家急性儿科危重症相关的住院负担和死亡率。
我们将使用医学主题词(MeSH)和关键词在MEDLINE、EMBASE、CINAHL和LILACS中检索符合条件的研究。结果将限于在低收入和中等收入国家住院的婴儿或儿童(年龄>28天至12岁)以及英文、西班牙文或法文出版物。排除非原始数据的出版物(如评论、社论、信件、笔记、会议材料)。
我们将纳入自2005年1月1日以来发表的符合所有纳入标准且能找到全文的观察性研究。
数据提取将包括与研究特征、医院特征、基础人群特征、患者人群特征和结局相关的信息。
我们将提取并报告关于研究、医院和患者特征、结局以及偏倚风险的数据。我们将按地区、国家收入水平和年龄报告入院原因和死亡率。当数据允许时,我们将报告或计算每种诊断的病死率(CFR)。
通过了解低收入和中等收入国家儿科危重症的负担,我们可以倡导资源,并为资源分配和投资决策提供信息,以改善低收入和中等收入国家急性儿科危重症患儿的管理和结局。