Division of Nephrology, Department of Medicine, Indiana University School of Medicine, Indianapolis, Indiana.
Department of Cellular and Integrative Physiology, Indiana University School of Medicine, Indianapolis, Indiana.
Physiol Rev. 2022 Oct 1;102(4):1625-1667. doi: 10.1152/physrev.00014.2021. Epub 2022 Apr 4.
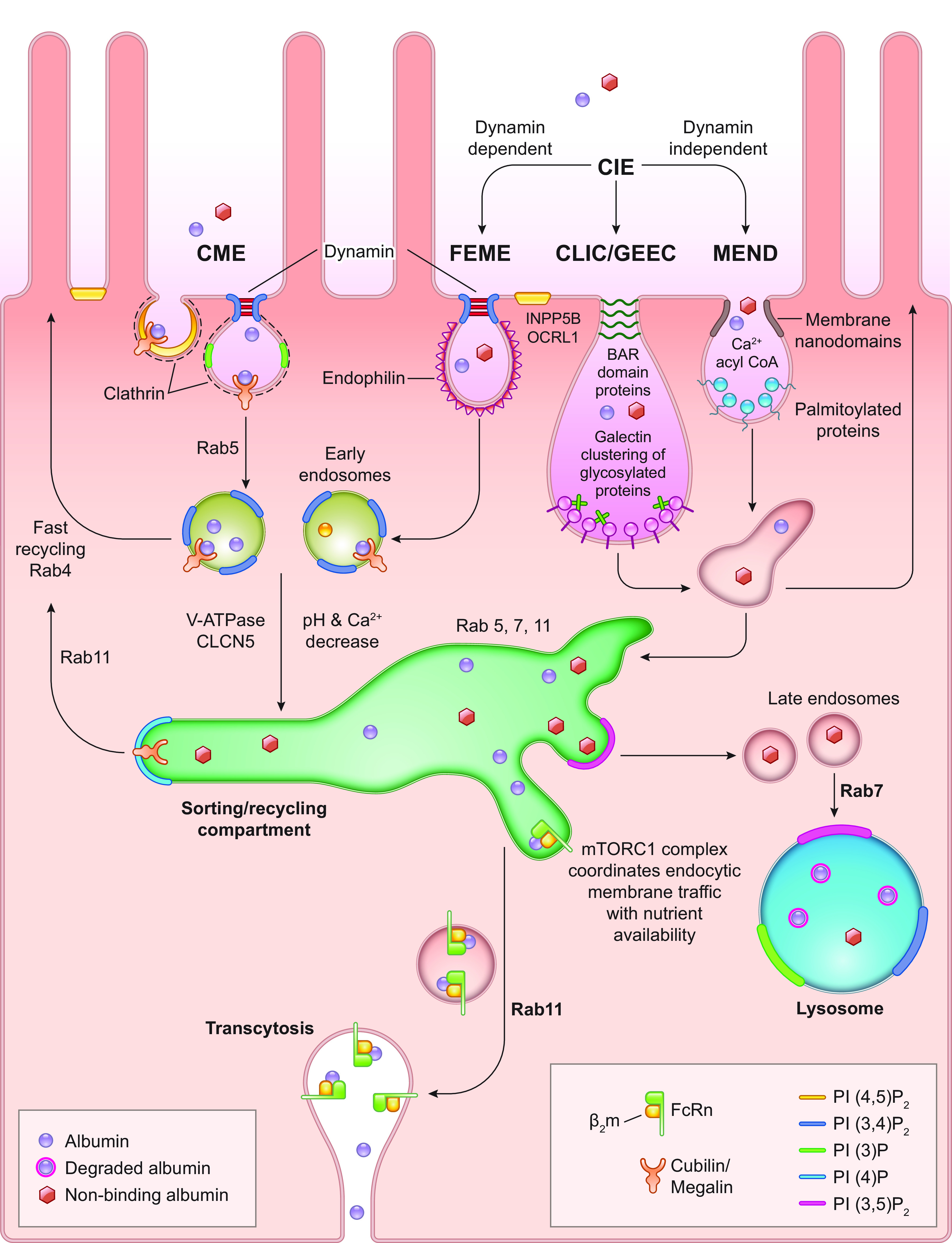
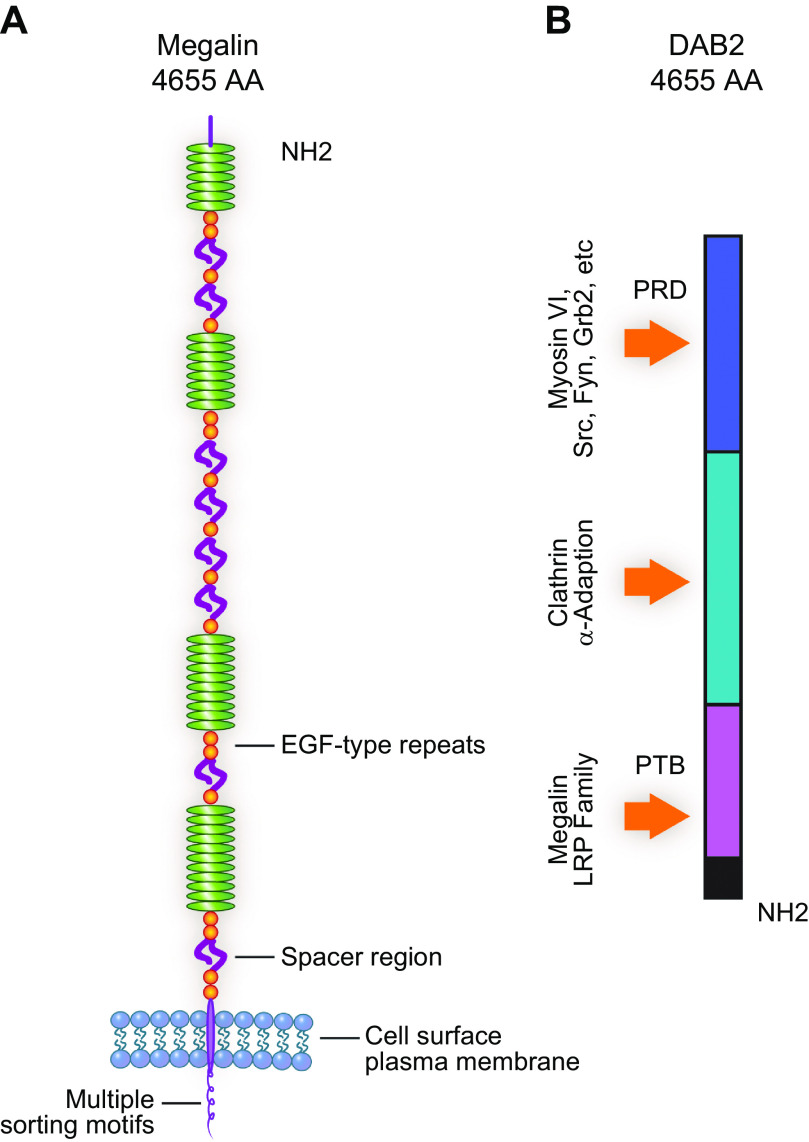
For nearly 50 years the proximal tubule (PT) has been known to reabsorb, process, and either catabolize or transcytose albumin from the glomerular filtrate. Innovative techniques and approaches have provided insights into these processes. Several genetic diseases, nonselective PT cell defects, chronic kidney disease (CKD), and acute PT injury lead to significant albuminuria, reaching nephrotic range. Albumin is also known to stimulate PT injury cascades. Thus, the mechanisms of albumin reabsorption, catabolism, and transcytosis are being reexamined with the use of techniques that allow for novel molecular and cellular discoveries. Megalin, a scavenger receptor, cubilin, amnionless, and Dab2 form a nonselective multireceptor complex that mediates albumin binding and uptake and directs proteins for lysosomal degradation after endocytosis. Albumin transcytosis is mediated by a pH-dependent binding affinity to the neonatal Fc receptor (FcRn) in the endosomal compartments. This reclamation pathway rescues albumin from urinary losses and cellular catabolism, extending its serum half-life. Albumin that has been altered by oxidation, glycation, or carbamylation or because of other bound ligands that do not bind to FcRn traffics to the lysosome. This molecular sorting mechanism reclaims physiological albumin and eliminates potentially toxic albumin. The clinical importance of PT albumin metabolism has also increased as albumin is now being used to bind therapeutic agents to extend their half-life and minimize filtration and kidney injury. The purpose of this review is to update and integrate evolving information regarding the reabsorption and processing of albumin by proximal tubule cells including discussion of genetic disorders and therapeutic considerations.
近 50 年来,人们已经知道近端肾小管(PT)从肾小球滤过液中重吸收、加工并代谢或转胞吞白蛋白。创新技术和方法为这些过程提供了新的见解。几种遗传疾病、非选择性 PT 细胞缺陷、慢性肾脏病(CKD)和急性 PT 损伤导致大量白蛋白尿,达到肾病范围。白蛋白也已知会刺激 PT 损伤级联反应。因此,正在使用允许进行新的分子和细胞发现的技术重新检查白蛋白重吸收、代谢和转胞吞的机制。巨球蛋白,一种清道夫受体, cubilin , amnionless ,和 Dab2 形成一个非选择性的多受体复合物,介导白蛋白结合和摄取,并在胞吞作用后将蛋白质导向溶酶体降解。白蛋白的转胞吞作用是通过与内体隔间中的新生 Fc 受体(FcRn)的 pH 依赖性结合亲和力介导的。这种回收途径从尿丢失和细胞代谢中拯救白蛋白,延长其血清半衰期。被氧化、糖化或氨甲酰化改变的白蛋白,或者因为其他不与 FcRn 结合的结合配体,会运送到溶酶体。这种分子分拣机制回收生理白蛋白并消除潜在的毒性白蛋白。PT 白蛋白代谢的临床重要性也随着白蛋白现在被用于结合治疗剂以延长其半衰期并最小化过滤和肾脏损伤而增加。本综述的目的是更新和整合有关近端肾小管细胞重吸收和加工白蛋白的不断发展的信息,包括讨论遗传疾病和治疗注意事项。