Marrero Humberto D J Gonzalez, Stålberg Erik V, Cooray Gerald, Corpeno Kalamgi Rebeca, Hedström Yvette, Bellander Bo-Michael, Nennesmo Inger, Larsson Lars
Section of Clinical Neurophysiology, Department of Clinical Neuroscience, Karolinska Institutet, 171 77 Stockholm, Sweden.
Department of Clinical Neurophysiology, Section of Neuroscience, Uppsala University, 751 85 Uppsala, Sweden.
Diagnostics (Basel). 2020 Nov 18;10(11):966. doi: 10.3390/diagnostics10110966.
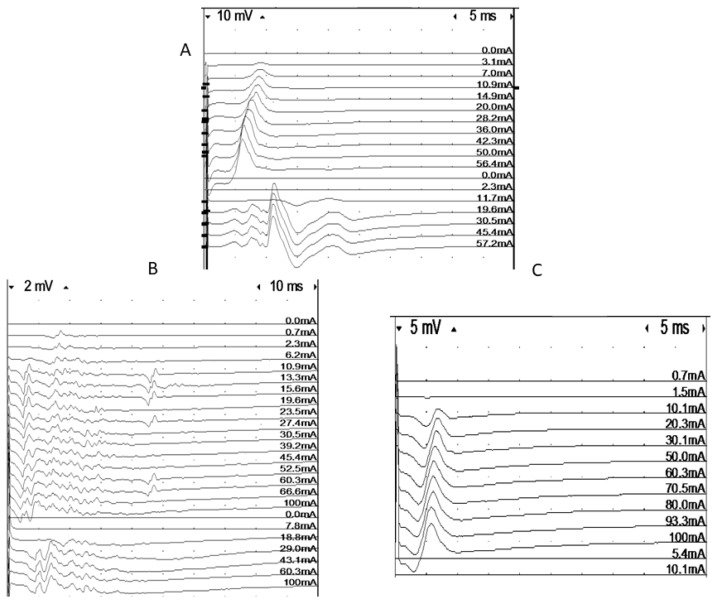
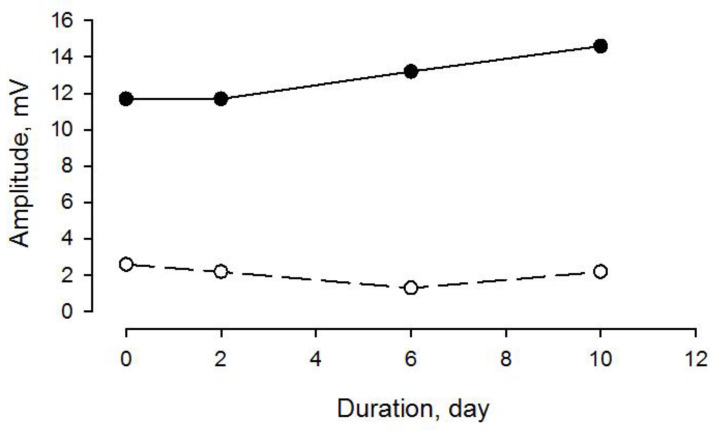
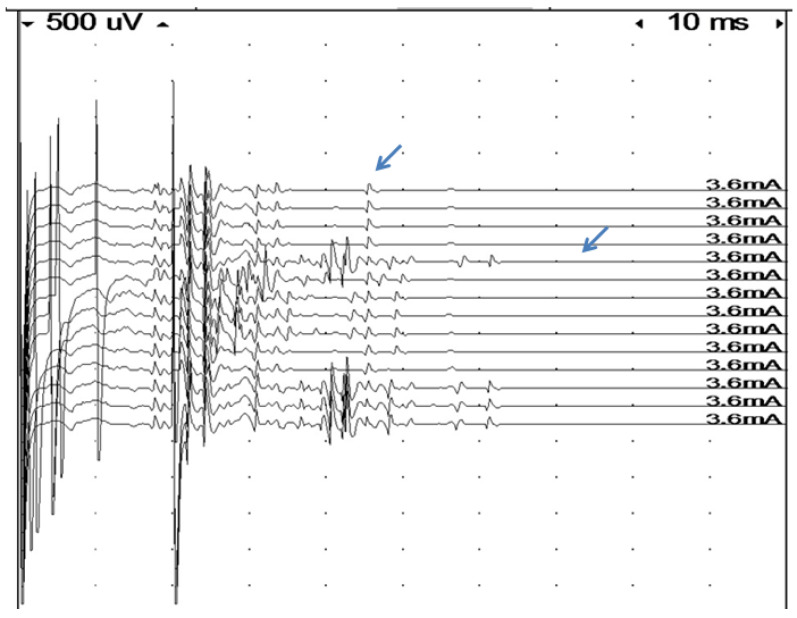
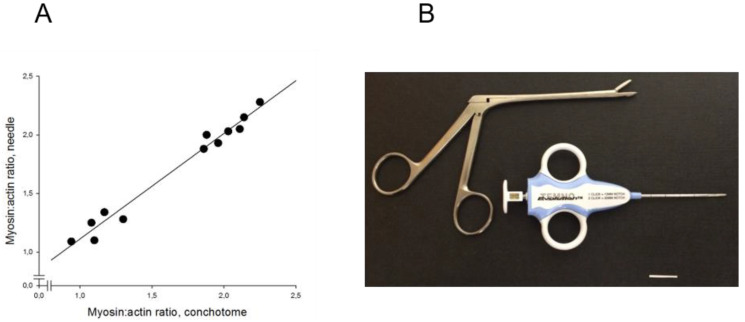
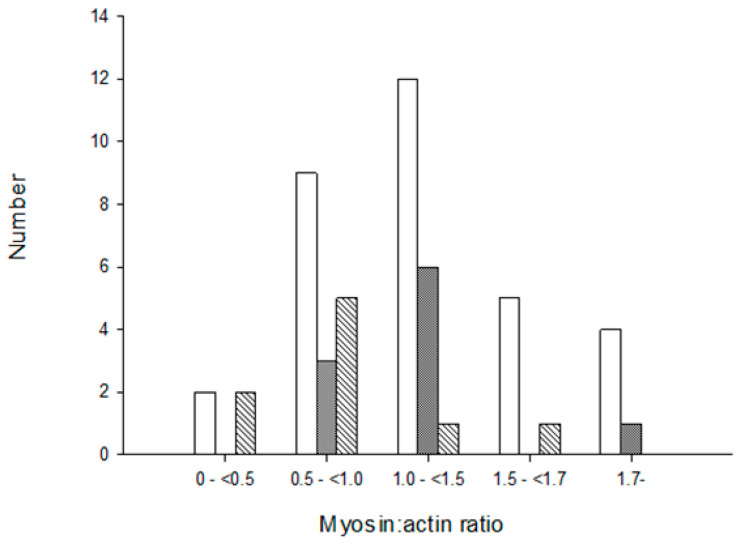
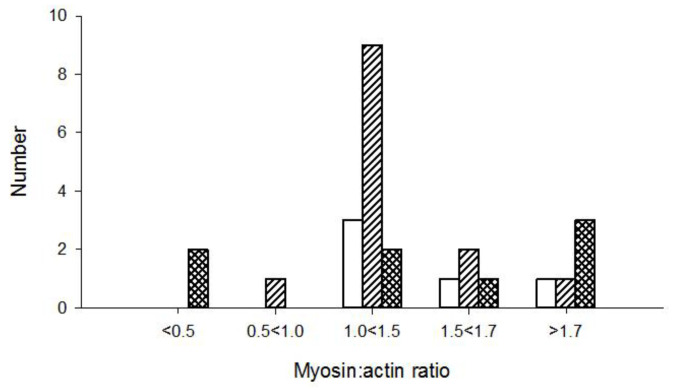
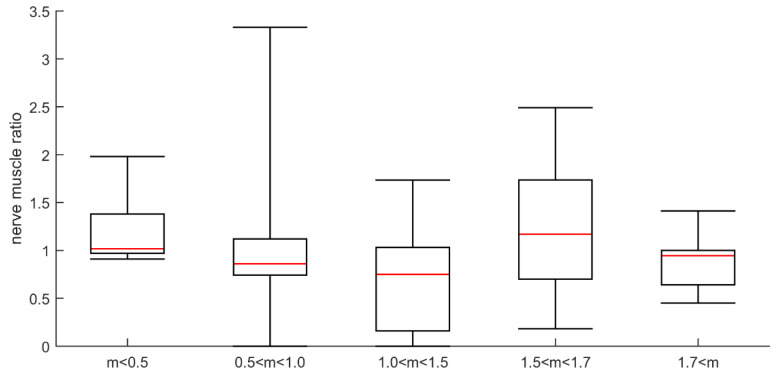
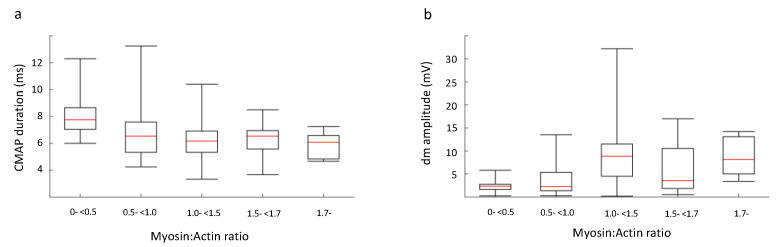
. The acquired muscle paralysis associated with modern critical care can be of neurogenic or myogenic origin, yet the distinction between these origins is hampered by the precision of current diagnostic methods. This has resulted in the pooling of all acquired muscle paralyses, independent of their origin, into the term Intensive Care Unit Acquired Muscle Weakness (ICUAW). This is unfortunate since the acquired neuropathy (critical illness polyneuropathy, CIP) has a slower recovery than the myopathy (critical illness myopathy, CIM); therapies need to target underlying mechanisms and every patient deserves as accurate a diagnosis as possible. This study aims at evaluating different diagnostic methods in the diagnosis of CIP and CIM in critically ill, immobilized and mechanically ventilated intensive care unit (ICU) patients. . ICU patients with acquired quadriplegia in response to critical care were included in the study. A total of 142 patients were examined with routine electrophysiological methods, together with biochemical analyses of myosin:actin (M:A) ratios of muscle biopsies. In addition, comparisons of evoked electromyographic (EMG) responses in direct vs. indirect muscle stimulation and histopathological analyses of muscle biopsies were performed in a subset of the patients. . ICU patients with quadriplegia were stratified into five groups based on the hallmark of CIM, i.e., preferential myosin loss (myosin:actin ratio, M:A) and classified as severe (M:A < 0.5; = 12), moderate (0.5 ≤ M:A < 1; = 40), mildly moderate (1 ≤ M:A < 1.5; = 49), mild (1.5 ≤ M:A < 1.7; = 24) and normal (1.7 ≤ M:A; = 19). Identical M:A ratios were obtained in the small (4-15 mg) muscle samples, using a disposable semiautomatic microbiopsy needle instrument, and the larger (>80 mg) samples, obtained with a conchotome instrument. Compound muscle action potential (CMAP) duration was increased and amplitude decreased in patients with preferential myosin loss, but deviations from this relationship were observed in numerous patients, resulting in only weak correlations between CMAP properties and M:A. Advanced electrophysiological methods measuring refractoriness and comparing CMAP amplitude after indirect nerve vs. direct muscle stimulation are time consuming and did not increase precision compared with conventional electrophysiological measurements in the diagnosis of CIM. Low CMAP amplitude upon indirect vs. direct stimulation strongly suggest a neurogenic lesion, i.e., CIP, but this was rarely observed among the patients in this study. Histopathological diagnosis of CIM/CIP based on enzyme histochemical mATPase stainings were hampered by poor quantitative precision of myosin loss and the impact of pathological findings unrelated to acute quadriplegia. . Conventional electrophysiological methods are valuable in identifying the peripheral origin of quadriplegia in ICU patients, but do not reliably separate between neurogenic vs. myogenic origins of paralysis. The hallmark of CIM, preferential myosin loss, can be reliably evaluated in the small samples obtained with the microbiopsy instrument. The major advantage of this method is that it is less invasive than conventional muscle biopsies, reducing the risk of bleeding in ICU patients, who are frequently receiving anticoagulant treatment, and it can be repeated multiple times during follow up for monitoring purposes.
与现代重症监护相关的后天性肌肉麻痹可能源于神经源性或肌源性,但目前诊断方法的精准度阻碍了对这些起源的区分。这导致所有后天性肌肉麻痹,无论其起源如何,都被归为重症监护病房获得性肌无力(ICUAW)这一术语。这很不幸,因为后天性神经病变(重症疾病多发性神经病,CIP)的恢复比肌病(重症疾病肌病,CIM)慢;治疗需要针对潜在机制,并且每个患者都应得到尽可能准确的诊断。本研究旨在评估不同诊断方法在诊断重症监护病房(ICU)中病情危重、卧床且接受机械通气的患者的CIP和CIM方面的效果。
本研究纳入了因重症监护而出现后天性四肢瘫痪的ICU患者。总共142例患者接受了常规电生理检查,并对肌肉活检样本进行了肌球蛋白:肌动蛋白(M:A)比率的生化分析。此外,对部分患者进行了直接与间接肌肉刺激诱发肌电图(EMG)反应的比较以及肌肉活检的组织病理学分析。
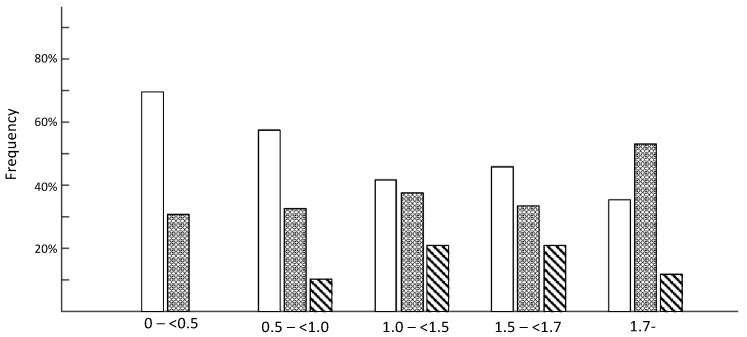
因四肢瘫痪的ICU患者根据CIM的特征,即肌球蛋白优先丢失(肌球蛋白:肌动蛋白比率,M:A)被分为五组,分别为重度(M:A < 0.5;n = 12)、中度(0.5 ≤ M:A < 1;n = 40)、轻度中度(1 ≤ M:A < 1.5;n = 49)、轻度(1.5 ≤ M:A < 1.7;n = 24)和正常(1.7 ≤ M:A;n = 19)。使用一次性半自动微生物活检针器械获取的小(4 - 15毫克)肌肉样本和使用鼻甲刀器械获取的大(>80毫克)样本获得了相同的M:A比率。肌球蛋白优先丢失的患者复合肌肉动作电位(CMAP)持续时间增加而幅度降低,但在许多患者中观察到了与这种关系的偏差,导致CMAP特性与M:A之间仅有微弱的相关性。在诊断CIM时,与传统电生理测量相比,测量不应期以及比较间接神经刺激与直接肌肉刺激后CMAP幅度的先进电生理方法耗时且并未提高诊断精度。间接与直接刺激时CMAP幅度低强烈提示神经源性病变,即CIP,但在本研究的患者中很少观察到这种情况。基于酶组织化学mATPase染色对CIM/CIP进行组织病理学诊断受到肌球蛋白丢失定量精度差以及与急性四肢瘫痪无关的病理结果影响的阻碍。
传统电生理方法在确定ICU患者四肢瘫痪的外周起源方面有价值,但不能可靠地区分瘫痪的神经源性与肌源性起源。CIM的特征,即肌球蛋白优先丢失,可以在使用微生物活检器械获取的小样本中可靠地评估。该方法的主要优点是它比传统肌肉活检侵入性小,可以降低经常接受抗凝治疗的ICU患者出血的风险,并且在随访期间可以多次重复进行以用于监测目的。