Center for Infectious Disease Imaging, Radiology and Imaging Sciences, Clinical Center, NIH, Bethesda, MD 20892.
Clinical Monitoring Research Program Directorate, Frederick National Laboratory for Cancer Research, National Cancer Institute, Frederick, MD 21702.
Proc Natl Acad Sci U S A. 2022 Apr 12;119(15):e2110846119. doi: 10.1073/pnas.2110846119. Epub 2022 Apr 6.
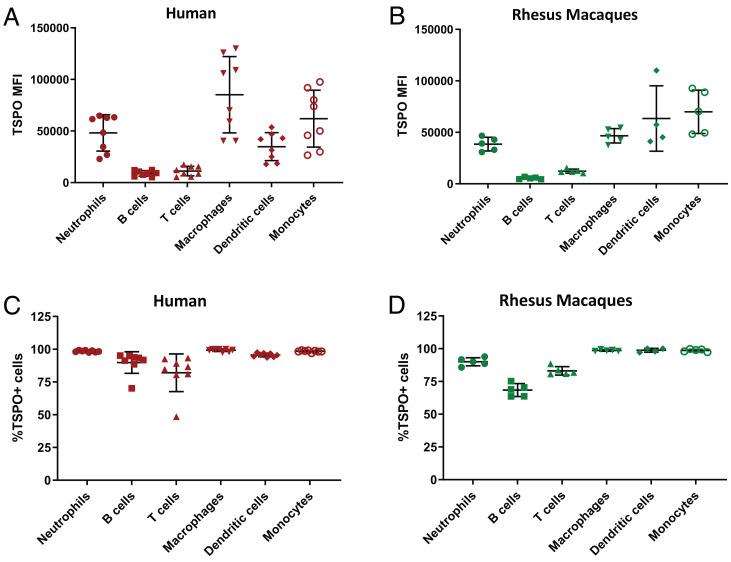
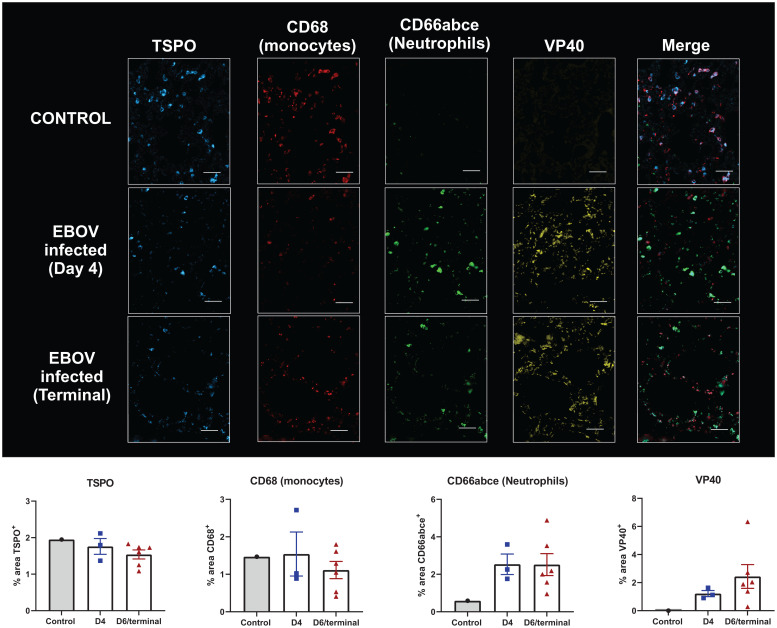
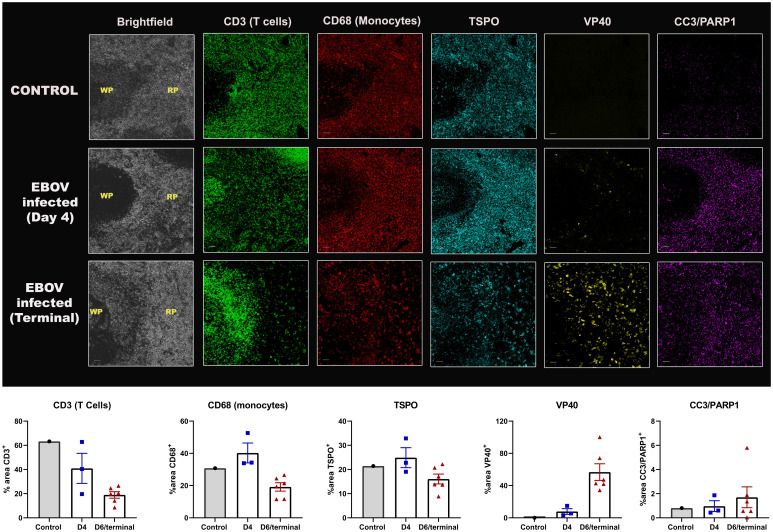
Ebola virus (EBOV) disease is characterized by lymphopenia, breach in vascular integrity, cytokine storm, and multiorgan failure. The pathophysiology of organ involvement, however, is incompletely understood. Using [18F]-DPA-714 positron emission tomography (PET) imaging targeting the translocator protein (TSPO), an immune cell marker, we sought to characterize the progression of EBOV-associated organ-level pathophysiology in the EBOV Rhesus macaque model. Dynamic [18F]-DPA-714 PET/computed tomography imaging was performed longitudinally at baseline and at multiple time points after EBOV inoculation, and distribution volumes (Vt) were calculated as a measure of peripheral TSPO binding. Using a mixed-effect linear regression model, spleen and lung Vt decreased, while the bone marrow Vt increased over time after infection. No clear trend was found for liver Vt. Multiple plasma cytokines correlated negatively with lung/spleen Vt and positively with bone marrow Vt. Multiplex immunofluorescence staining in spleen and lung sections confirmed organ-level lymphoid and monocytic loss/apoptosis, thus validating the imaging results. Our findings are consistent with EBOV-induced progressive monocytic and lymphocytic depletion in the spleen, rather than immune activation, as well as depletion of alveolar macrophages in the lungs, with inefficient reactive neutrophilic activation. Increased bone marrow Vt, on the other hand, suggests hematopoietic activation in response to systemic immune cell depletion and leukocytosis and could have prognostic relevance. In vivo PET imaging provided better understanding of organ-level pathophysiology during EBOV infection. A similar approach can be used to delineate the pathophysiology of other systemic infections and to evaluate the effectiveness of newly developed treatment and vaccine strategies.
埃博拉病毒(EBOV)病的特征是淋巴细胞减少、血管完整性受损、细胞因子风暴和多器官衰竭。然而,器官受累的病理生理学尚不完全清楚。我们使用靶向转位蛋白(TSPO)的[18F]-DPA-714 正电子发射断层扫描(PET)成像来研究 EBOV 恒河猴模型中 EBOV 相关器官水平病理生理学的进展,TSPO 是一种免疫细胞标志物。在 EBOV 接种前后的多个时间点进行动态[18F]-DPA-714 PET/计算机断层扫描成像,并计算分布容积(Vt)作为外周 TSPO 结合的衡量标准。使用混合效应线性回归模型,感染后脾和肺 Vt 随时间降低,而骨髓 Vt 增加。肝 Vt 没有明显趋势。多个血浆细胞因子与肺/脾 Vt 呈负相关,与骨髓 Vt 呈正相关。脾和肺组织切片的多重免疫荧光染色证实了器官水平的淋巴细胞和单核细胞缺失/凋亡,从而验证了成像结果。我们的发现与 EBOV 诱导的脾内进行性单核细胞和淋巴细胞耗竭一致,而不是免疫激活,以及肺内肺泡巨噬细胞耗竭,伴有低效的反应性中性粒细胞激活。骨髓 Vt 的增加则表明骨髓造血在全身免疫细胞耗竭和白细胞增多的情况下被激活,可能具有预后相关性。体内 PET 成像为了解 EBOV 感染期间的器官水平病理生理学提供了更好的认识。类似的方法可用于描绘其他全身感染的病理生理学,并评估新开发的治疗和疫苗策略的有效性。