Zhang Xiao-Yan, Cai Si-Man, Zhang Li, Zhu Qing-Li, Sun Qiang, Jiang Yu-Xin, Wang Hong-Yan, Li Jian-Chu
Department of Diagnostic Ultrasound, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, China.
Department of Breast Surgery, Peking Union Medical College Hospital, Chinese Academy of Medical Sciences, Beijing, China.
Front Oncol. 2022 Mar 21;12:861151. doi: 10.3389/fonc.2022.861151. eCollection 2022.
To determine whether vascular index (VI; defined as the ratio of Doppler signal pixels to pixels in the total lesion) measured superb microvascular imaging in breast cancer correlates with immunohistochemically defined subtype and is able to predict molecular subtypes.
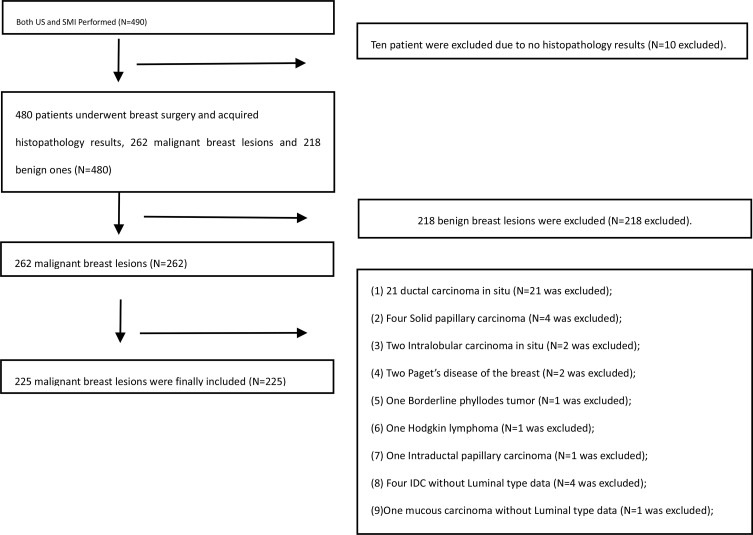
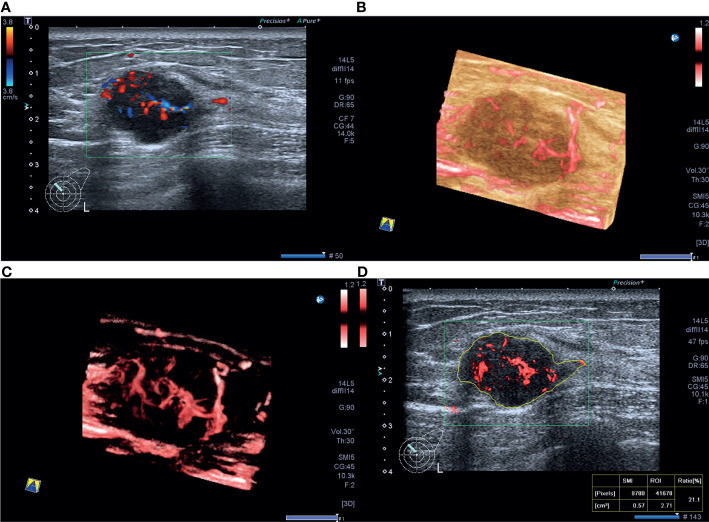
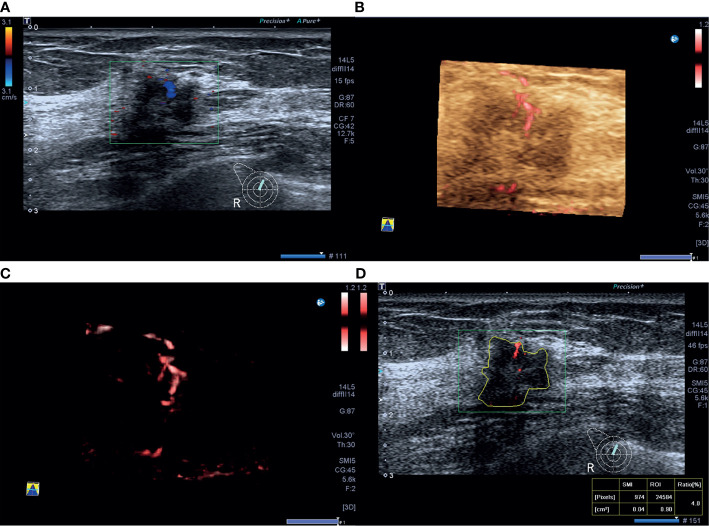
This prospective study involved 225 patients with 225 mass-type invasive breast cancers (mean size 2.6 ± 1.4 cm, range 0.4~5.9 cm) who underwent ultrasound and superb microvascular imaging (SMI) at Peking Union Medical College Hospital before breast surgery from December 2016 to June 2018. The correlations between primary tumor VI measured SMI, clinicopathological findings, and molecular subtype were analyzed. The performance of VI for prediction of molecular subtypes in invasive breast cancer was investigated.
The median VI of the 225 tumors was 7.3% (4.2%11.8%) (range 0%54.4%). Among the subtypes of the 225 tumors, 41 (18.2%) were luminal A, 91 (40.4%) were luminal B human epidermal growth factor receptor-2 (HER-2)-negative, 26 (11.6%) were luminal B HER-2-positive, 17 (7.6%) were HER-2-positive, and 50 (22.2%) were triple-negative, and the corresponding median VI values were 5.9% (2.6%11.6%) (range 0%47.1%), 7.3 (4.4%10.5%) (range 0%29.5%), 6.3% (3.9%11.3%) (range 0.6%22.2%), 8.2% (4.9%15.6%) (range 0.9%54.4%), and 9.2% (5.1%15.3%) (range 0.7%32.9%), respectively. Estrogen receptor (ER) negativity, higher tumor grade, and higher Ki-67 index (≥20%) were significantly associated with a higher VI value. Tumor size, ER status, and Ki-67 index were shown to independently influence VI. A cutoff value of 4.1% yielded 79.9% sensitivity and 41.5% specificity with an area under the receiver operating characteristic curve (AUC) of 0.58 for predicting that a tumor was of the luminal A subtype. A cutoff value of 16.4% yielded 30.0% sensitivity and 90.3% specificity with an AUC of 0.60 for predicting a triple-negative subtype.
VI, as a quantitative index obtained by SMI examination, could reflect histologic vascular changes in invasive breast cancer and was found to be higher in more biologically aggressive breast tumors. VI shows a certain degree of correlation with the molecular subtype of invasive breast cancer and plays a limited role in predicting the luminal A with high sensitivity and triple-negative subtype with high specificity.
确定在乳腺癌中通过超声造影微血管成像测量的血管指数(VI,定义为多普勒信号像素与整个病变像素之比)是否与免疫组化定义的亚型相关,并能够预测分子亚型。
这项前瞻性研究纳入了225例患有225个肿块型浸润性乳腺癌的患者(平均大小2.6±1.4 cm,范围0.4~5.9 cm),这些患者于2016年12月至2018年6月在北京协和医院接受乳房手术前接受了超声和超声造影微血管成像(SMI)检查。分析了通过SMI测量的原发性肿瘤VI、临床病理特征和分子亚型之间的相关性。研究了VI在预测浸润性乳腺癌分子亚型方面的性能。
225个肿瘤的VI中位数为7.3%(4.2%11.8%)(范围0%54.4%)。在225个肿瘤的亚型中,41个(18.2%)为腔面A型,91个(40.4%)为腔面B型人表皮生长因子受体2(HER-2)阴性,26个(11.6%)为腔面B型HER-2阳性,17个(7.6%)为HER-2阳性,50个(22.2%)为三阴性,相应的VI中位数分别为5.9%(2.6%11.6%)(范围0%47.1%)、7.3(4.4%10.5%)(范围0%29.5%)、6.3%(3.9%11.3%)(范围 .6%22.2%)、8.2%(4.9%15.6%)(范围0.9%54.4%)和9.2%(5.1%15.3%)(范围0.7%32.9%)。雌激素受体(ER)阴性、更高的肿瘤分级和更高的Ki-67指数(≥20%)与更高的VI值显著相关。肿瘤大小、ER状态和Ki-67指数被证明独立影响VI。预测肿瘤为腔面A型时,截断值为4.1%时敏感性为79.9%,特异性为41.5%,受试者工作特征曲线(AUC)下面积为0.58。预测三阴性亚型时,截断值为16.4%时敏感性为30.0%,特异性为90.3%,AUC为0.60。
VI作为通过SMI检查获得的定量指标,可以反映浸润性乳腺癌的组织学血管变化,并且在生物学行为更具侵袭性的乳腺肿瘤中更高。VI与浸润性乳腺癌的分子亚型显示出一定程度的相关性,在高敏感性预测腔面A型和高特异性预测三阴性亚型方面发挥有限作用。