Galli Maria Giulia, Djuric Olivera, Besutti Giulia, Ottone Marta, Amidei Lucia, Bitton Lee, Bonilauri Carlotta, Boracchia Luca, Campanale Sergio, Curcio Vittoria, Lucchesi Davide Maria Francesco, Mulas Cesare Salvatore, Santi Francesca, Ferrari Anna Maria, Giorgi Rossi Paolo, Luppi Francesco
Emergency Department, Azienda USL - IRCCS di Reggio Emilia, Reggio Emilia, Emilia-Romagna, Italy.
Epidemiology Unit, Azienda USL - IRCCS di Reggio Emilia, Reggio Emilia, Emilia-Romagna, Italy.
BMJ Open. 2022 Apr 6;12(4):e052665. doi: 10.1136/bmjopen-2021-052665.
We aimed at identifying baseline predictive factors for emergency department (ED) readmission, with hospitalisation/death, in patients with COVID-19 previously discharged from the ED. We also developed a disease progression velocity index.
Retrospective cohort study of prospectively collected data. The charts of consecutive patients with COVID-19 discharged from the Reggio Emilia (Italy) ED (2 March 2 to 31 March 2020) were retrospectively examined. Clinical, laboratory and CT findings at first ED admission were tested as predictive factors using multivariable logistic models. We divided CT extension by days from symptom onset to build a synthetic velocity index.
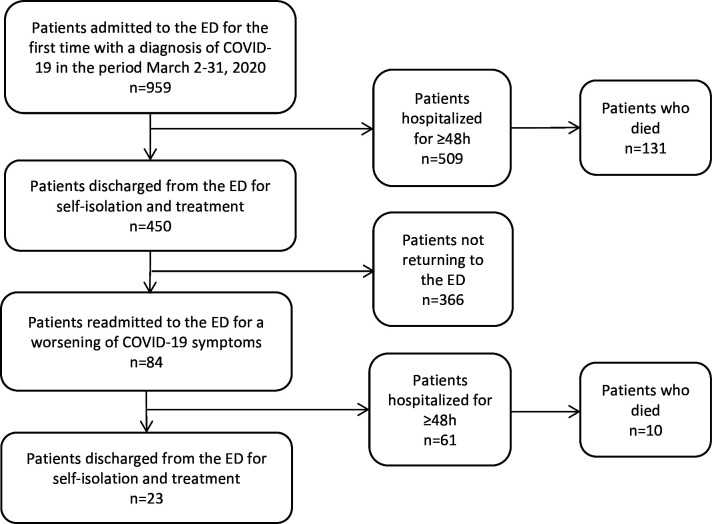
450 patients discharged from the ED with diagnosis of COVID-19.
ED readmission within 14 days, followed by hospitalisation/death.
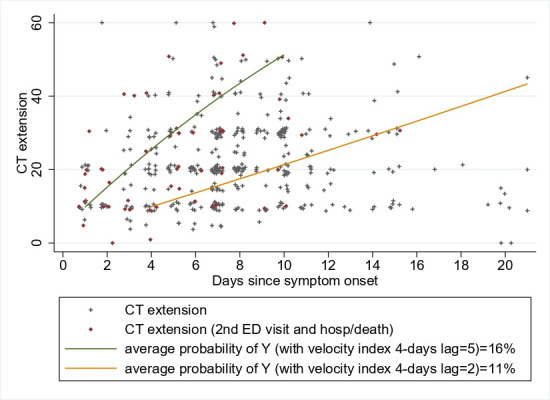
Of the discharged patients, 84 (18.7%) were readmitted to the ED, 61 (13.6%) were hospitalised and 10 (2.2%) died. Age (OR=1.05; 95% CI 1.03 to 1.08), Charlson Comorbidity Index 3 versus 0 (OR=11.61; 95% CI 1.76 to 76.58), days from symptom onset (OR for 1-day increase=0.81; 95% CI 0.73 to 0.90) and CT extension (OR for 1% increase=1.03; 95% CI 1.01 to 1.06) were associated in a multivariable model for readmission with hospitalisation/death. A 2-day lag velocity index was a strong predictor (OR for unit increase=1.21, 95% CI 1.08 to 1.36); the model including this index resulted in less information loss.
A velocity index combining CT extension and days from symptom onset predicts disease progression in patients with COVID-19. For example, a 20% CT extension 3 days after symptom onset has the same risk as does 50% after 10 days.
我们旨在确定急诊科(ED)出院的COVID-19患者再次入住急诊科并伴有住院/死亡情况的基线预测因素。我们还开发了一种疾病进展速度指数。
对前瞻性收集的数据进行回顾性队列研究。对意大利雷焦艾米利亚急诊科(2020年3月2日至3月31日)连续出院的COVID-19患者的病历进行回顾性检查。使用多变量逻辑模型将首次急诊科入院时的临床、实验室和CT检查结果作为预测因素进行测试。我们用症状出现到CT扩展的天数来构建一个综合速度指数。
450例诊断为COVID-19并从急诊科出院的患者。
14天内再次入住急诊科,随后住院/死亡。
出院患者中,84例(18.7%)再次入住急诊科,61例(13.6%)住院,10例(2.2%)死亡。年龄(比值比[OR]=1.05;95%置信区间[CI]1.03至1.08)、查尔森合并症指数3与0(OR=11.61;95%CI 1.76至76.58)、症状出现后的天数(每增加1天的OR=0.81;95%CI 0.73至0.90)和CT扩展(每增加1%的OR=1.03;95%CI 1.01至1.06)在再次入住急诊科并伴有住院/死亡情况的多变量模型中具有相关性。2天滞后速度指数是一个强有力的预测因素(单位增加的OR=1.21,95%CI 1.08至1.36);包含该指数的模型导致的信息损失更少。
结合CT扩展和症状出现天数的速度指数可预测COVID-19患者的疾病进展。例如,症状出现3天后CT扩展20%与10天后CT扩展50%具有相同风险。