Clinical and Experimental Medicine PhD Program, University of Modena and Reggio Emilia, Modena, Italy.
Radiology Unit, Department of Diagnostic Imaging and Laboratory Medicine, AUSL-IRCCS di Reggio Emilia, Via Risorgimento 80, 42123, Reggio Emilia, Italy.
Eur Radiol. 2021 Dec;31(12):9164-9175. doi: 10.1007/s00330-021-07993-9. Epub 2021 May 12.
The aims of this study were to develop a multiparametric prognostic model for death in COVID-19 patients and to assess the incremental value of CT disease extension over clinical parameters.
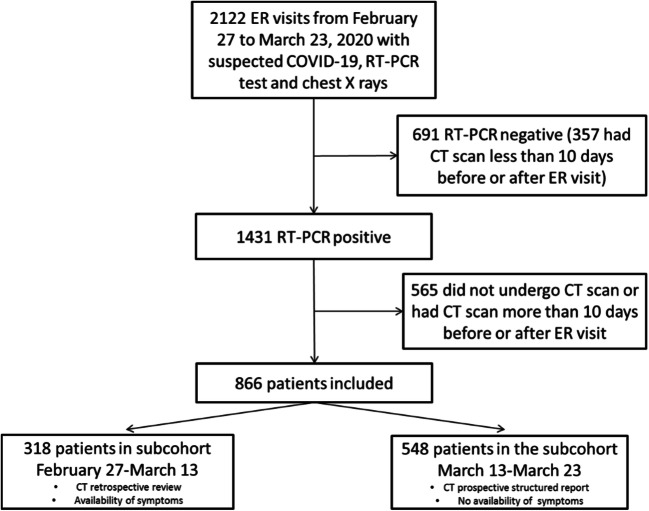
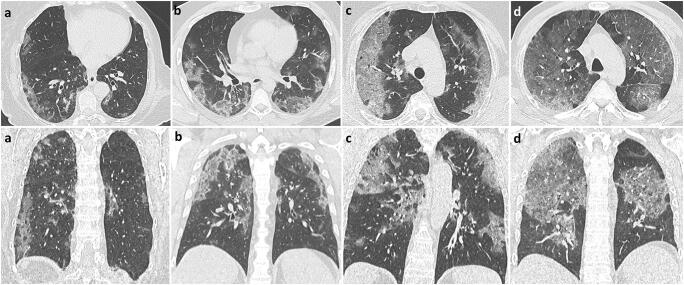
Consecutive patients who presented to all five of the emergency rooms of the Reggio Emilia province between February 27 and March 23, 2020, for suspected COVID-19, underwent chest CT, and had a positive swab within 10 days were included in this retrospective study. Age, sex, comorbidities, days from symptom onset, and laboratory data were retrieved from institutional information systems. CT disease extension was visually graded as < 20%, 20-39%, 40-59%, or ≥ 60%. The association between clinical and CT variables with death was estimated with univariable and multivariable Cox proportional hazards models; model performance was assessed using k-fold cross-validation for the area under the ROC curve (cvAUC).
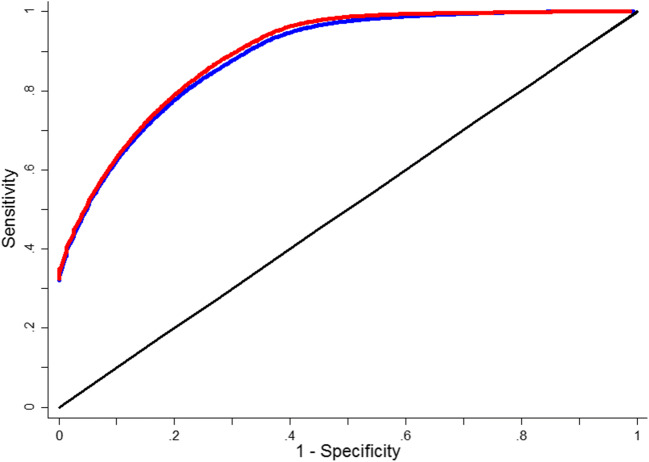
Of the 866 included patients (median age 59.8, women 39.2%), 93 (10.74%) died. Clinical variables significantly associated with death in multivariable model were age, male sex, HDL cholesterol, dementia, heart failure, vascular diseases, time from symptom onset, neutrophils, LDH, and oxygen saturation level. CT disease extension was also independently associated with death (HR = 7.56, 95% CI = 3.49; 16.38 for ≥ 60% extension). cvAUCs were 0.927 (bootstrap bias-corrected 95% CI = 0.899-0.947) for the clinical model and 0.936 (bootstrap bias-corrected 95% CI = 0.912-0.953) when adding CT extension.
A prognostic model based on clinical variables is highly accurate in predicting death in COVID-19 patients. Adding CT disease extension to the model scarcely improves its accuracy.
• Early identification of COVID-19 patients at higher risk of disease progression and death is crucial; the role of CT scan in defining prognosis is unclear. • A clinical model based on age, sex, comorbidities, days from symptom onset, and laboratory results was highly accurate in predicting death in COVID-19 patients presenting to the emergency room. • Disease extension assessed with CT was independently associated with death when added to the model but did not produce a valuable increase in accuracy.
本研究旨在建立一个针对 COVID-19 患者死亡的多参数预后模型,并评估 CT 疾病扩展相对于临床参数的增量价值。
本回顾性研究纳入了 2020 年 2 月 27 日至 3 月 23 日期间因疑似 COVID-19 而前往雷焦艾米利亚省五个急诊室的连续患者,这些患者均接受了胸部 CT 检查,并且在 10 天内进行了阳性拭子检测。从机构信息系统中检索年龄、性别、合并症、症状出现后天数和实验室数据。通过视觉评分将 CT 疾病扩展分为<20%、20-39%、40-59%或≥60%。使用单变量和多变量 Cox 比例风险模型估计临床和 CT 变量与死亡之间的关联;使用 K 折交叉验证评估 ROC 曲线下面积(cvAUC)的模型性能。
在 866 名纳入患者中(中位年龄 59.8 岁,女性占 39.2%),有 93 人(10.74%)死亡。多变量模型中与死亡显著相关的临床变量包括年龄、男性、高密度脂蛋白胆固醇、痴呆、心力衰竭、血管疾病、症状出现后时间、中性粒细胞、乳酸脱氢酶和氧饱和度水平。CT 疾病扩展也与死亡独立相关(HR=7.56,95%CI=3.49;16.38 为≥60%扩展)。临床模型的 cvAUC 为 0.927(自举偏置校正 95%CI=0.899-0.947),添加 CT 扩展后为 0.936(自举偏置校正 95%CI=0.912-0.953)。
基于临床变量的预后模型在预测 COVID-19 患者死亡方面具有很高的准确性。在模型中添加 CT 疾病扩展几乎不会提高其准确性。
早期识别 COVID-19 患者中疾病进展和死亡风险较高的患者至关重要;CT 扫描在确定预后方面的作用尚不清楚。
基于年龄、性别、合并症、症状出现后时间和实验室结果的临床模型在预测 COVID-19 患者就诊急诊室时的死亡方面具有很高的准确性。
通过 CT 评估的疾病扩展与死亡独立相关,但添加到模型中并未产生有价值的准确性提高。