URRIS-UR2CA, Centre Hospitalier Universitaire de Nice, Nice, France.
Département de Médecine Interne, Centre Hospitalier Universitaire de Nice, Nice, France.
Front Immunol. 2022 Mar 25;13:864133. doi: 10.3389/fimmu.2022.864133. eCollection 2022.
Many patients are referred to multiple sclerosis (MS) tertiary centers to manage brain white matter hyperintensities (WMH). Multiple diagnoses can match in such situations, and we lack proper tools to diagnose complex cases.
This study aimed to prospectively analyze and correlate with the final diagnosis, cerebrospinal fluid (CSF) interleukin (IL)-1β, soluble IL-2 receptor (CD25), IL-6, IL-10, and kappa free light chains (KFLC) concentrations in patients presenting with brain WMH.
All patients over 18 years addressed to our MS tertiary center for the diagnostic workup of brain WMH were included from June 1, 2020, to June 1, 2021. Patients were separated into three groups-MS and related disorder (MSARD), other inflammatory neurological disorder (OIND), and non-inflammatory neurological disorder (NIND) groups-according to clinical presentation, MRI characteristics, and biological workup.
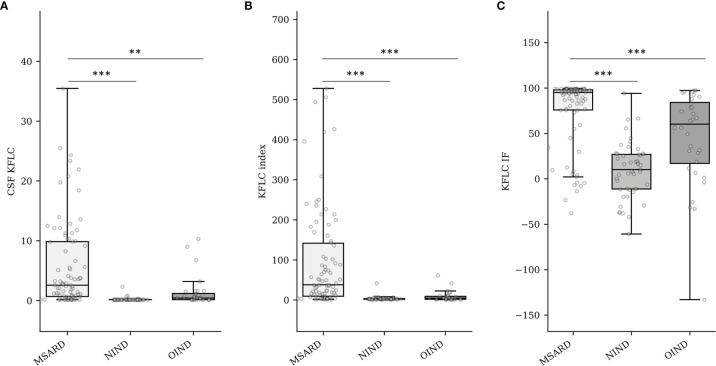
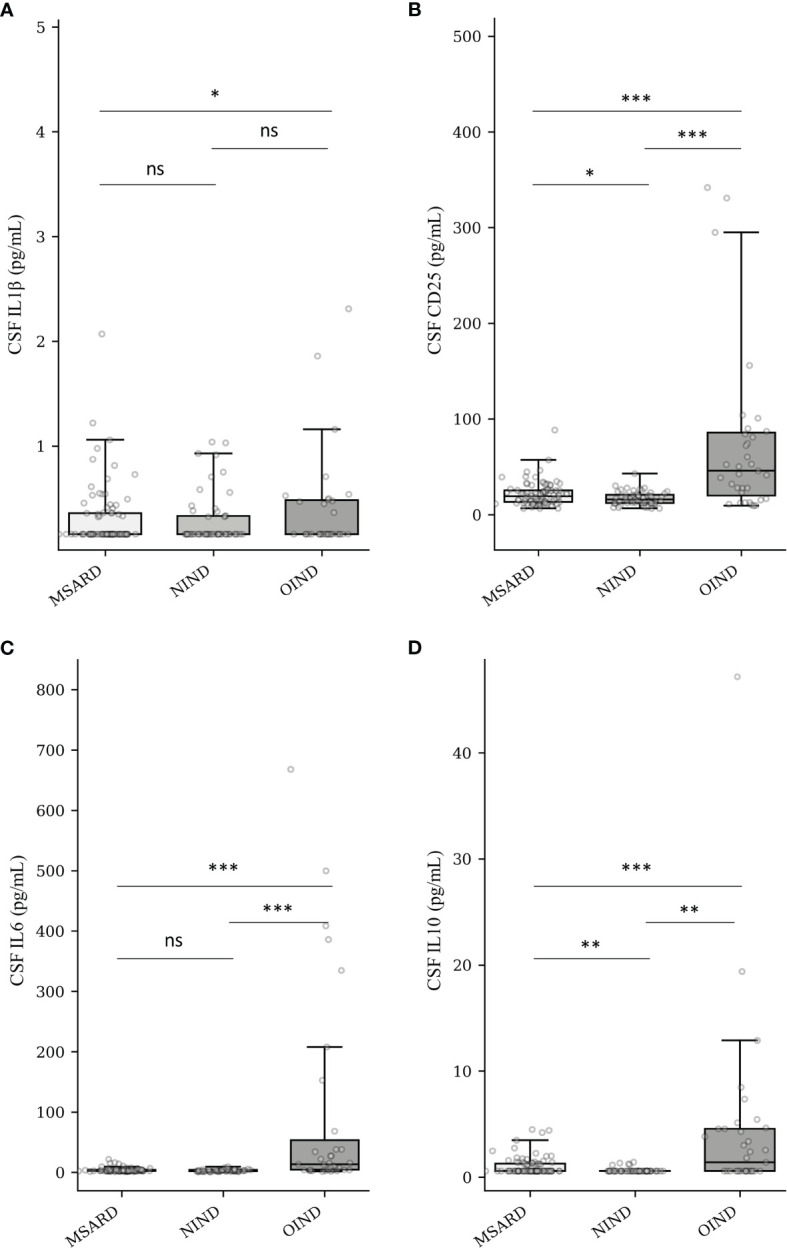
A total of 176 patients (129 women, mean age 45.8 ± 14.7 years) were included. The diagnosis was MSARD ( = 88), OIND ( = 35), and NIND ( = 53). Median CSF KFLC index and KFLC intrathecal fraction (IF) were higher in MSARD than in the OIND and NIND groups; < 0.001 for all comparisons. CSF CD25 and IL-6 concentrations were higher in the OIND group than in both the MSARD and NIND groups; < 0.001 for all comparisons. KFLC index could rule in MSARD when compared to NIND (sensitivity, 0.76; specificity, 0.91) or OIND (sensitivity, 0.73; specificity, 0.76). These results were similar to those with oligoclonal bands (sensitivity, 0.59; specificity, 0.98 compared to NIND; sensitivity, 0.59; specificity, 0.88 compared to OIND). In contrast, elevated CSF CD25 and IL-6 could rule out MSARD when compared to OIND (sensitivity, 0.58 and 0.88; specificity, 0.95 and 0.74, respectively).
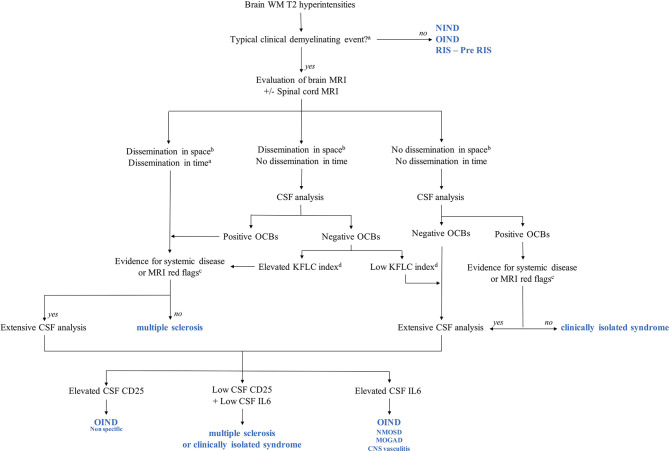
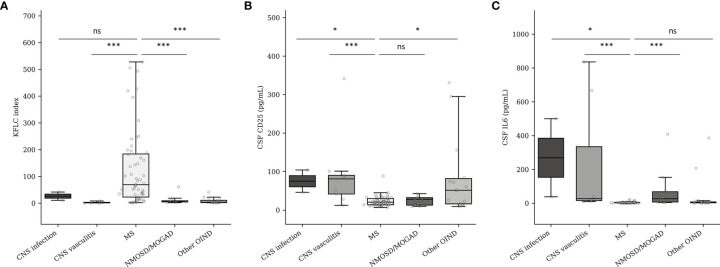
Our results show that, as OCBs, KFLC biomarkers are helpful tools to rule in MSARD, whereas elevated CSF CD25 and IL-6 rule out MSARD. Interestingly, CSF IL-6 concentration could help identify neuromyelitis optica spectrum disorder, myelin oligodendrocyte glycoprotein antibody-associated disease, and central nervous system (CNS) vasculitis. These results need to be confirmed within more extensive and multicentric studies. Still, they sustain that KFLC, CSF CD25, and CSF IL-6 could be reliable biomarkers in brain WMH diagnostic workup for differentiating MSARD from other brain inflammatory MS mimickers.
许多患者被转诊到多发性硬化症(MS)三级中心以治疗脑白质高信号(WMH)。在这种情况下,可能会出现多种诊断结果相匹配的情况,而我们缺乏诊断复杂病例的适当工具。
本研究旨在前瞻性分析并与最终诊断相关联,对表现为脑 WMH 的患者的脑脊液(CSF)白细胞介素(IL)-1β、可溶性 IL-2 受体(CD25)、IL-6、IL-10 和游离轻链 K(KFLC)浓度进行分析。
2020 年 6 月 1 日至 2021 年 6 月 1 日期间,所有因脑 WMH 诊断而到我们 MS 三级中心就诊的年龄在 18 岁以上的患者均被纳入本研究。根据临床表现、MRI 特征和生物学检查,将患者分为三组——MS 及相关疾病(MSARD)、其他炎症性神经疾病(OIND)和非炎症性神经疾病(NIND)组。
共纳入 176 例患者(129 例女性,平均年龄 45.8±14.7 岁)。诊断为 MSARD(n=88)、OIND(n=35)和 NIND(n=53)。MSARD 患者的 CSF KFLC 指数和 KFLC 鞘内分数(IF)中位数高于 OIND 和 NIND 组;所有比较均为 <0.001。OIND 组的 CSF CD25 和 IL-6 浓度高于 MSARD 和 NIND 组;所有比较均为 <0.001。与 NIND 或 OIND 相比,KFLC 指数可用于诊断 MSARD(灵敏度分别为 0.76 和 0.73,特异性分别为 0.91 和 0.76)。这些结果与寡克隆带(灵敏度分别为 0.59 和 0.59,特异性分别为 0.98 和 0.88)相似。相比之下,与 OIND 相比,升高的 CSF CD25 和 IL-6 可排除 MSARD(灵敏度分别为 0.58 和 0.88,特异性分别为 0.95 和 0.74)。
我们的研究结果表明,与 OCB 一样,KFLC 生物标志物是有助于诊断 MSARD 的有用工具,而升高的 CSF CD25 和 IL-6 可排除 MSARD。有趣的是,CSF IL-6 浓度有助于识别视神经脊髓炎谱系疾病、髓鞘少突胶质细胞糖蛋白抗体相关疾病和中枢神经系统(CNS)血管炎。这些结果需要在更广泛和多中心的研究中进行验证。尽管如此,它们仍然表明 KFLC、CSF CD25 和 CSF IL-6 可能是脑 WMH 诊断中区分 MSARD 与其他脑炎症性 MS 模拟物的可靠生物标志物。