Oxford Vaccine Group, Department of Paediatrics, University of Oxford, Oxford, UK.
NIHR Southampton Clinical Research Facility and Biomedical Research Centre, University Hospital Southampton NHS Foundation Trust, Southampton, UK; Faculty of Medicine and Institute for Life Sciences, University of Southampton, Southampton, UK.
J Infect. 2022 Jun;84(6):795-813. doi: 10.1016/j.jinf.2022.04.018. Epub 2022 Apr 9.
To evaluate the persistence of immunogenicity three months after third dose boosters.
COV-BOOST is a multicentre, randomised, controlled, phase 2 trial of seven COVID-19 vaccines used as a third booster dose. The analysis was conducted using all randomised participants who were SARS-CoV-2 naïve during the study.
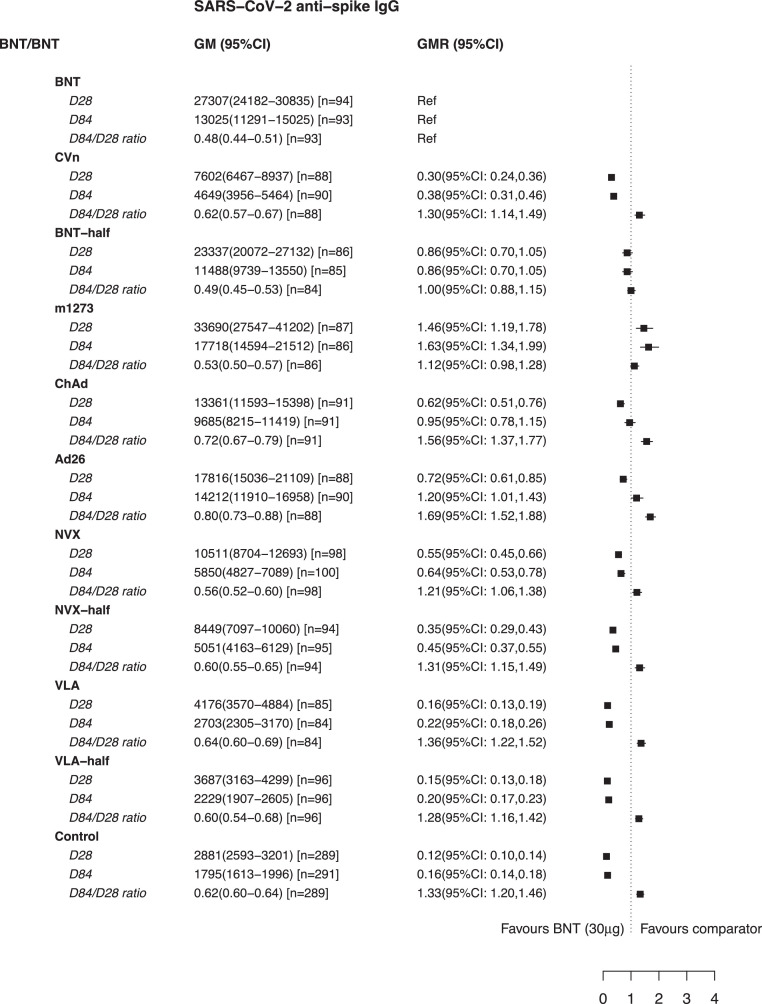
Amongst the 2883 participants randomised, there were 2422 SARS-CoV-2 naïve participants until D84 visit included in the analysis with median age of 70 (IQR: 30-94) years. In the participants who had two initial doses of ChAdOx1 nCov-19 (Oxford-AstraZeneca; hereafter referred to as ChAd), schedules using mRNA vaccines as third dose have the highest anti-spike IgG at D84 (e.g. geometric mean concentration of 8674 ELU/ml (95% CI: 7461-10,085) following ChAd/ChAd/BNT162b2 (Pfizer-BioNtech, hearafter referred to as BNT)). However, in people who had two initial doses of BNT there was no significant difference at D84 in people given ChAd versus BNT (geometric mean ratio (GMR) of 0.95 (95%CI: 0.78, 1.15). Also, people given Ad26.COV2.S (Janssen; hereafter referred to as Ad26) as a third dose had significantly higher anti-spike IgG at D84 than BNT (GMR of 1.20, 95%CI: 1.01,1.43). Responses at D84 between people who received BNT (15 μg) or BNT (30 μg) after ChAd/ChAd or BNT/BNT were similar, with anti-spike IgG GMRs of half-BNT (15 μg) versus BNT (30 μg) ranging between 0.74-0.86. The decay rate of cellular responses were similar between all the vaccine schedules and doses.
84 days after a third dose of COVID-19 vaccine the decay rates of humoral response were different between vaccines. Adenoviral vector vaccine anti-spike IgG concentrations at D84 following BNT/BNT initial doses were similar to or even higher than for a three dose (BNT/BNT/BNT) schedule. Half dose BNT immune responses were similar to full dose responses. While high antibody tires are desirable in situations of high transmission of new variants of concern, the maintenance of immune responses that confer long-lasting protection against severe disease or death is also of critical importance. Policymakers may also consider adenoviral vector, fractional dose of mRNA, or other non-mRNA vaccines as third doses.
评估第三剂加强针接种后三个月的免疫原性持久性。
COV-BOOST 是一项评估七种 COVID-19 疫苗作为第三剂加强针使用的多中心、随机、对照、2 期临床试验。该分析使用了所有在研究期间对 SARS-CoV-2 呈初次感染状态的随机参与者。
在 2883 名随机分配的参与者中,有 2422 名 SARS-CoV-2 初次感染参与者在 D84 访视时纳入分析,中位年龄为 70(IQR:30-94)岁。在接受 ChAdOx1 nCov-19(牛津-阿斯利康;以下简称 ChAd)两剂初始疫苗接种的参与者中,使用 mRNA 疫苗作为第三剂的方案在 D84 时具有最高的抗刺突 IgG(例如,ChAd/ChAd/BNT162b2(辉瑞-生物技术,以下简称 BNT)后抗刺突 IgG 的几何平均浓度为 8674 ELU/ml(95%CI:7461-10085)。然而,在接受两剂初始 BNT 接种的人群中,在接受 ChAd 与 BNT 接种的人群中,在 D84 时并无显著差异(几何均数比值(GMR)为 0.95(95%CI:0.78,1.15)。此外,接受 Ad26.COV2.S(杨森;以下简称 Ad26)作为第三剂的人群在 D84 时具有比 BNT 更高的抗刺突 IgG(GMR 为 1.20,95%CI:1.01,1.43)。在 D84 时,接受 ChAd/ChAd 或 BNT/BNT 后接受 BNT(15μg)或 BNT(30μg)接种的人群之间的细胞应答率相似,半剂量 BNT(15μg)与 BNT(30μg)之间的抗刺突 IgG GMR 范围在 0.74-0.86 之间。所有疫苗接种方案和剂量的细胞应答衰减率相似。
在 COVID-19 疫苗接种第三剂后 84 天,不同疫苗的体液免疫应答衰减率不同。在接受 BNT/BNT 初始接种后,腺病毒载体疫苗的抗刺突 IgG 浓度与三剂(BNT/BNT/BNT)方案相似或甚至更高。BNT 的半剂量免疫应答与全剂量应答相似。虽然在新关注的变异体高传播情况下高抗体滴度是理想的,但保持对严重疾病或死亡具有长期保护作用的免疫应答也至关重要。决策者可能还会考虑腺病毒载体、mRNA 疫苗的分数剂量或其他非 mRNA 疫苗作为第三剂。