Prassas Dimitrios, Safi Sami Alexander, Stylianidi Maria Chara, Telan Leila Anne, Krieg Sarah, Roderburg Christoph, Esposito Irene, Luedde Tom, Knoefel Wolfram Trudo, Krieg Andreas
Department of Surgery (A), Heinrich-Heine-University and University Hospital Duesseldorf, Moorenstr. 5, 40225 Duesseldorf, Germany.
Clinic for Gastroenterology, Hepatology and Infectious Diseases, Heinrich-Heine-University and University Hospital Duesseldorf, Moorenstr. 5, 40225 Duesseldorf, Germany.
Cancers (Basel). 2022 Apr 6;14(7):1834. doi: 10.3390/cancers14071834.
Even though numerous novel lymph node (LN) classification schemes exist, an extensive comparison of their performance in patients with resected pancreatic ductal adenocarcinoma (PDAC) has not yet been performed.
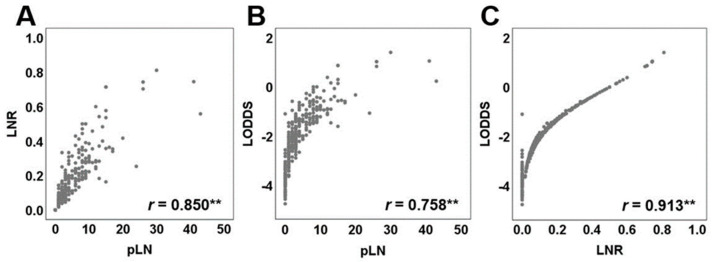
We investigated the prognostic performance and discriminative ability of 25 different LN ratio (LNR) and 27 log odds of metastatic LN (LODDS) classifications by means of Cox regression and C-statistic in 319 patients with resected PDAC. Regression models were adjusted for age, sex, T category, grading, localization, presence of metastatic disease, positivity of resection margins, and neoadjuvant therapy.
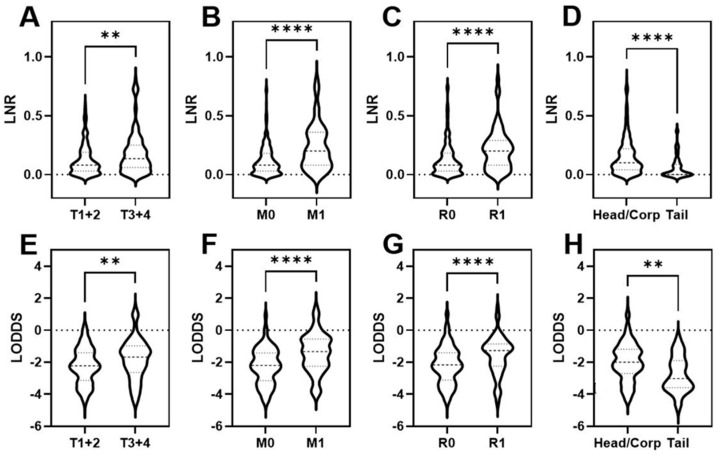
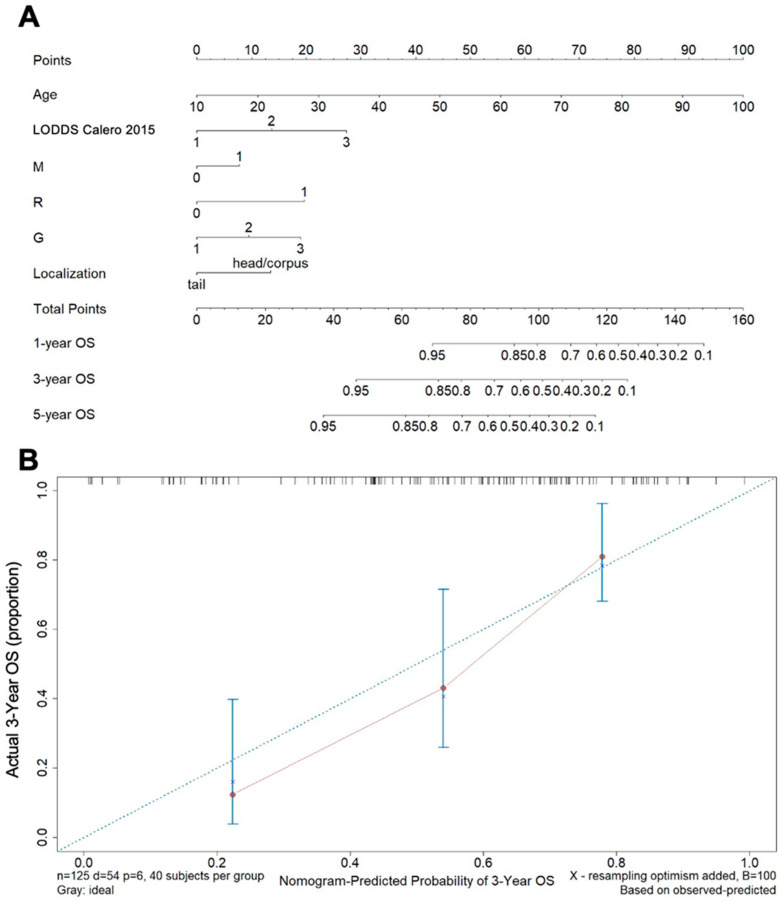
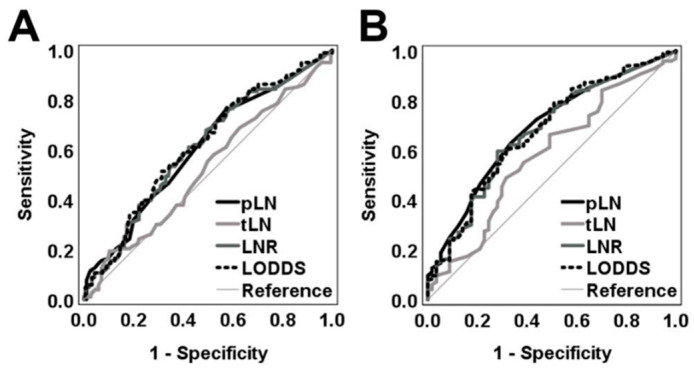
Both LNR or LODDS as continuous variables were associated with advanced tumor stage, distant metastasis, positive resection margins, and PDAC of the head or corpus. Two distinct LN classifications, one LODDS and one LNR, were found to be superior to the N category in the complete patient collective. However, only the LODDS classification exhibited statistically significant, gradually increasing HRs of their subcategories and at the same time significantly higher discriminative potential in the subgroups of patients with PDAC of the head or corpus and in patients with tumor free resection margins or M0 status, respectively. On this basis, we built a clinically helpful nomogram to estimate the prognosis of patients after radically resected PDAC.
One LNR and one LODDS classification scheme were found to out-perform the N category in terms of both prognostic performance and discriminative ability, in distinct patient subgroups, with reference to OS in patients with resected PDAC.
尽管存在众多新颖的淋巴结(LN)分类方案,但尚未对其在接受胰腺导管腺癌(PDAC)切除术患者中的性能进行广泛比较。
我们通过Cox回归和C统计量,在319例接受PDAC切除术的患者中,研究了25种不同的淋巴结比率(LNR)和27种转移性淋巴结对数优势(LODDS)分类的预后性能和判别能力。回归模型根据年龄、性别、T分期、分级、定位、转移性疾病的存在、切缘阳性和新辅助治疗进行了调整。
LNR或LODDS作为连续变量均与肿瘤晚期、远处转移、切缘阳性以及胰头或胰体部的PDAC相关。在整个患者群体中,发现两种不同的LN分类,一种是LODDS,一种是LNR,优于N分期。然而,只有LODDS分类在其亚组中显示出具有统计学意义的、逐渐增加的风险比(HRs),并且同时在胰头或胰体部PDAC患者亚组以及切缘无肿瘤或M0状态患者亚组中分别具有显著更高的判别潜力。在此基础上,我们构建了一个对临床有帮助的列线图,以估计接受根治性切除的PDAC患者的预后。
就预后性能和判别能力而言,在不同的患者亚组中,参照接受PDAC切除术患者的总生存期(OS),发现一种LNR和一种LODDS分类方案优于N分期。