Department of Clinical Pharmacy and Pharmacology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands.
Unit of Clinical Epidemiology, "Città della Salute e della Scienza" Hospital and CPO Piemonte, Turin, Italy.
Acta Diabetol. 2022 Jul;59(7):949-957. doi: 10.1007/s00592-022-01891-2. Epub 2022 Apr 21.
Valid health economic models are essential to inform the adoption and reimbursement of therapies for diabetes mellitus. Often existing health economic models are applied in other countries and settings than those where they were developed. This practice requires assessing the transferability of a model developed from one setting to another. We evaluate the transferability of the MICADO model, developed for the Dutch 2007 setting, in two different settings using a range of adjustment steps. MICADO predicts micro- and macrovascular events at the population level.
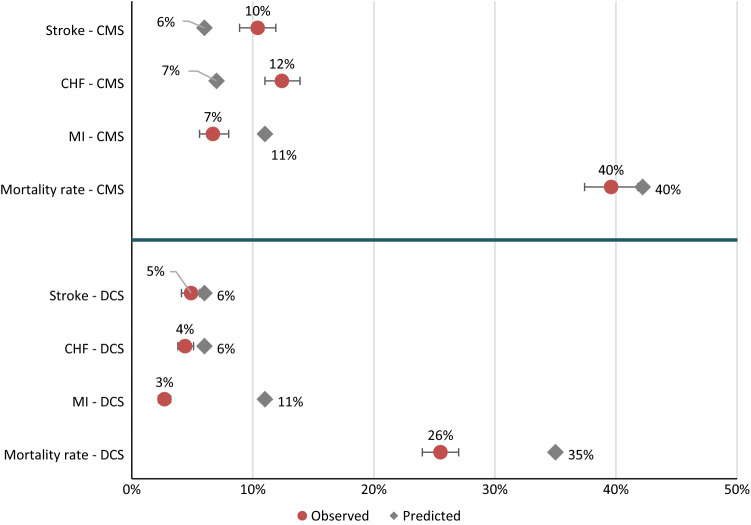
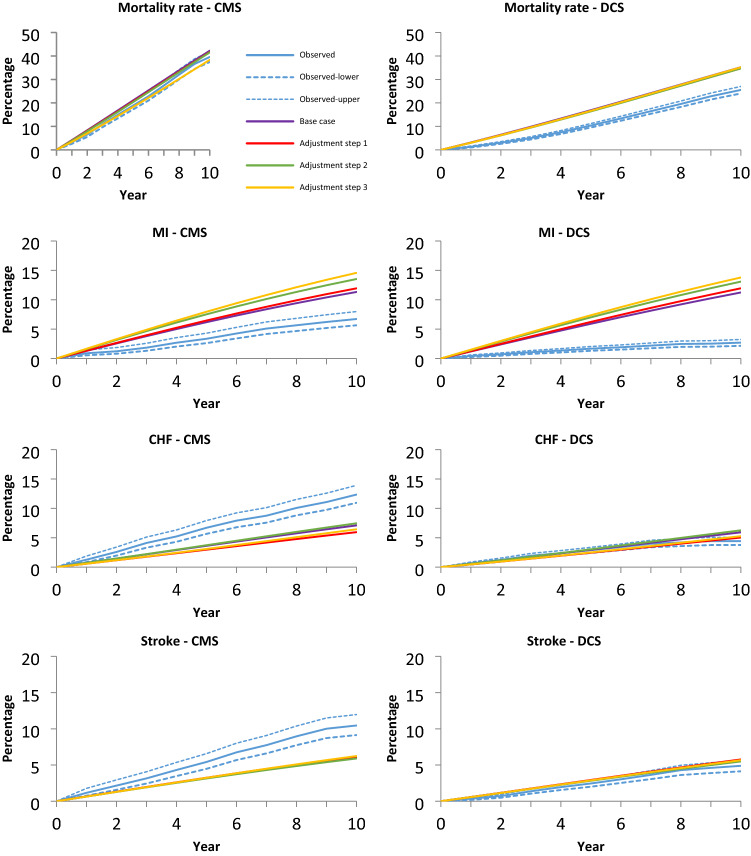
MICADO simulation results were compared to observed events in an Italian 2000-2015 cohort (Casale Monferrato Survey [CMS]) and in a Dutch 2008-2019 (Hoorn Diabetes Care Center [DCS]) cohort after adjusting the demographic characteristics. Additional adjustments were performed to: (1) risk factors prevalence at baseline, (2) prevalence of complications, and (3) all-cause mortality risks by age and sex. Model validity was assessed by mean average percentage error (MAPE) of cumulative incidences over 10 years of follow-up, where lower values mean better accuracy.
For mortality, MAPE was lower for CMS compared to DCS (0.38 vs. 0.70 following demographic adjustment) and adjustment step 3 improved it to 0.20 in CMS, whereas step 2 showed best results in DCS (0.65). MAPE for heart failure and stroke in DCS were 0.11 and 0.22, respectively, while for CMS was 0.42 and 0.41.
The transferability of the MICADO model varied by event and per cohort. Additional adjustments improved prediction of events for MICADO. To ensure a valid model in a new setting it is imperative to assess the impact of adjustments in terms of model accuracy, even when this involves the same country, but a new time period.
有效的健康经济模型对于为糖尿病治疗提供信息的采用和报销至关重要。通常,现有的健康经济模型是在开发它们的国家和环境之外的其他国家和环境中应用的。这种做法需要评估从一个环境到另一个环境转移模型的能力。我们使用一系列调整步骤评估了为 2007 年荷兰制定的 MICADO 模型在两个不同环境中的可转移性。MICADO 预测人群水平的微血管和大血管事件。
将 MICADO 模拟结果与意大利 2000-2015 年队列(卡萨尔蒙费拉托调查 [CMS])和荷兰 2008-2019 年(霍恩糖尿病护理中心 [DCS])队列的观察事件进行比较,对人口统计学特征进行调整后。进行了额外的调整,以:(1)基线时的风险因素流行率,(2)并发症的流行率,以及(3)按年龄和性别划分的全因死亡率风险。通过 10 年随访累积发生率的平均平均百分比误差(MAPE)评估模型的有效性,较低的值表示更高的准确性。
对于死亡率,CMS 中的 MAPE 低于 DCS(人口统计学调整后分别为 0.38 和 0.70),调整步骤 3 将其提高到 CMS 中的 0.20,而调整步骤 2 在 DCS 中显示出最佳结果(0.65)。DCS 中心心力衰竭和中风的 MAPE 分别为 0.11 和 0.22,而 CMS 中心的 MAPE 分别为 0.42 和 0.41。
MICADO 模型的可转移性因事件和每个队列而异。额外的调整改善了 MICADO 对事件的预测。为了确保在新环境中使用有效的模型,必须根据模型准确性评估调整的影响,即使涉及同一个国家,但处于新的时间段也是如此。