Wienemann Hendrik, Langenbach Marcel C, Mauri Victor, Banazadeh Maryam, Klein Konstantin, Hohmann Christopher, Lee Samuel, Breidert Isabel, Hof Alexander, Eghbalzadeh Kaveh, Kuhn Elmar, Halbach Marcel, Maintz David, Baldus Stephan, Bunck Alexander, Adam Matti
Clinic III for Internal Medicine, Faculty of Medicine and University Hospital Cologne, University of Cologne, Kerpener Str. 61, 50937 Cologne, Germany.
Department of Radiology, Faculty of Medicine and University Hospital Cologne, University of Cologne, Kerpener Str. 61, 50937 Cologne, Germany.
J Cardiovasc Dev Dis. 2022 Apr 14;9(4):116. doi: 10.3390/jcdd9040116.
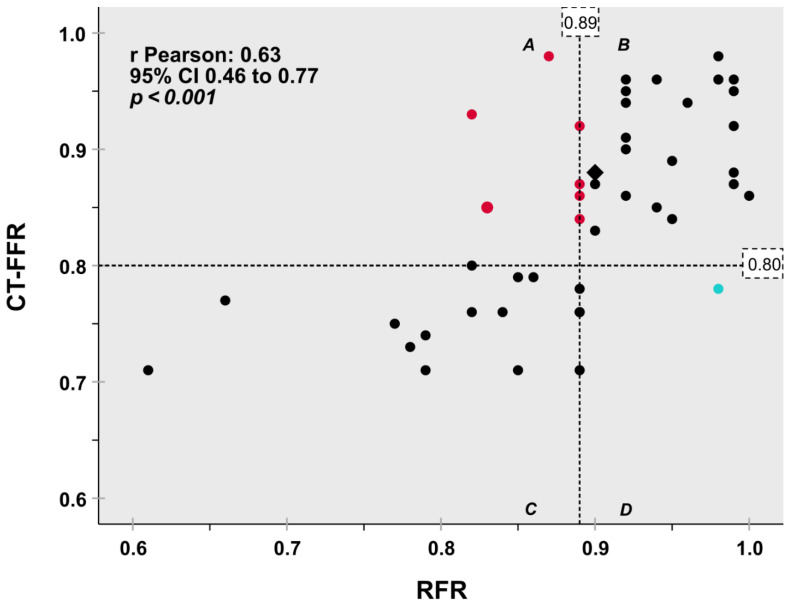
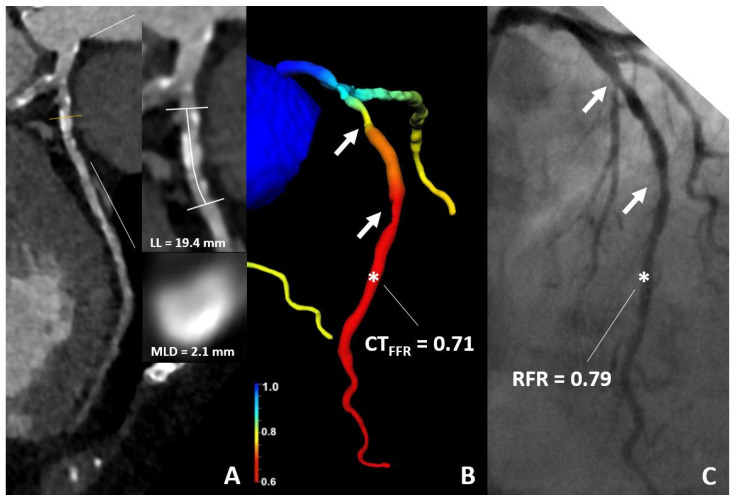
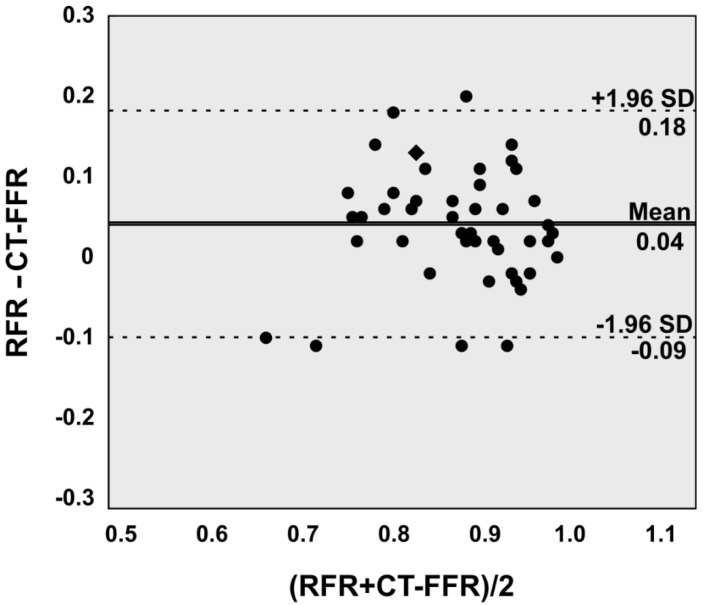
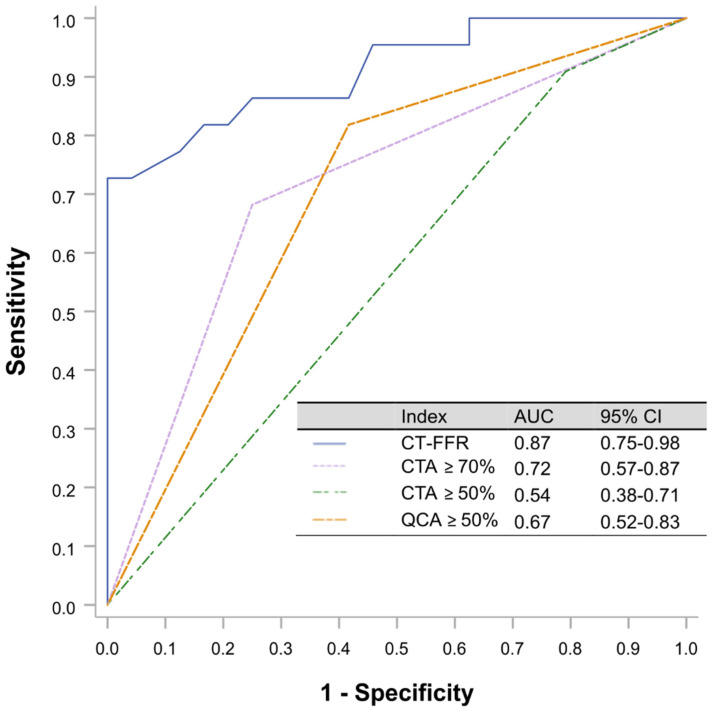
Background: Computed tomography derived Fractional Flow Reserve (CT-FFR) has been shown to decrease the referral rate for invasive coronary angiography (ICA). The purpose of the study was to evaluate the diagnostic performance of CT-FFR compared to hyperemia-free index Resting Full-cycle Ratio (RFR) in patients with relevant aortic stenosis (AS) and intermediate coronary stenosis. Methods: 41 patients with 46 coronary lesions underwent ICA with quantitative coronary angiography (QCA), pressure wire assessment and routine pre-transcatheter aortic valve replacement (TAVR) computed tomography (CT). CT-FFR analysis was performed using prototype on-site software. Results: RFR showed a significant correlation with CT-FFR (Pearson’s correlation, r = 0.632, p < 0.001). On a per-lesion basis, diagnostic accuracy, sensitivity, specificity, positive predictive value, and negative predictive value of CT-FFR were 82.6% (95% CI 68.6−92.2), 69.6% (95% CI 47.1−86.8), 95.7% (95% CI 78.1−99.9), 94.1% (95% CI 69.8−99.1), and 75.9% (95% CI 62.7−85.4), respectively. The optimal cutoff value of the CT-FFR for RFR ≤ 0.89 prediction was 0.815. The area under the receiver curve showed a larger area under the curve for CT-FFR (0.87; 95% CI 0.75−0.98) compared with CTA stenosis of ≥50% (0.54, 95% CI 0.38−0.71), CTA ≥ 70% (0.72, 95% CI 0.57−0.87) and QCA ≥ 50% (0.67, 95% CI 0.52−0.83). Conclusions: CT-FFR assessed by routine pre-TAVR CT is safe and feasible and shows a significant correlation with RFR in patients with AS. CT-FFR is superior to QCA ≥ 50%, CT ≥ 50% and CT ≥ 70% in assessing the hemodynamic relevance of intermediate coronary lesions. Thus, CT-FFR has the potential to guide revascularization in patients with AS.
计算机断层扫描衍生的血流储备分数(CT-FFR)已被证明可降低侵入性冠状动脉造影(ICA)的转诊率。本研究的目的是评估在有相关主动脉瓣狭窄(AS)和中度冠状动脉狭窄的患者中,CT-FFR与无充血指数静息全周期比率(RFR)相比的诊断性能。方法:41例有46处冠状动脉病变的患者接受了ICA检查,包括定量冠状动脉造影(QCA)、压力导丝评估和经导管主动脉瓣置换术(TAVR)前的常规计算机断层扫描(CT)。使用现场原型软件进行CT-FFR分析。结果:RFR与CT-FFR显示出显著相关性(Pearson相关性,r = 0.632,p < 0.001)。基于每个病变,CT-FFR的诊断准确性、敏感性、特异性、阳性预测值和阴性预测值分别为82.6%(95%可信区间68.6−92.2)、69.6%(95%可信区间47.1−86.8)、95.7%(95%可信区间78.1−99.9)、94.1%(95%可信区间69.8−99.1)和75.9%(95%可信区间62.7−85.4)。对于RFR≤0.89预测,CT-FFR的最佳截断值为0.815。与CTA狭窄≥50%(0.54,95%可信区间0.38−0.71)、CTA≥70%(0.72,95%可信区间0.57−0.87)和QCA≥50%(0.67,95%可信区间0.52−0.83)相比,CT-FFR的受试者工作特征曲线下面积更大(0.87;95%可信区间0.75−0.98)。结论:TAVR术前常规CT评估的CT-FFR是安全可行的,并且在AS患者中与RFR显示出显著相关性。在评估中度冠状动脉病变的血流动力学相关性方面,CT-FFR优于QCA≥50%、CT≥50%和CT≥70%。因此,CT-FFR有潜力指导AS患者的血运重建。