Gohmann Robin F, Schug Adrian, Krieghoff Christian, Seitz Patrick, Majunke Nicolas, Buske Maria, Kaiser Fyn, Schaudt Sebastian, Renatus Katharina, Desch Steffen, Leontyev Sergey, Noack Thilo, Kiefer Philipp, Pawelka Konrad, Lücke Christian, Abdelhafez Ahmed, Ebel Sebastian, Borger Michael A, Thiele Holger, Panknin Christoph, Abdel-Wahab Mohamed, Horn Matthias, Gutberlet Matthias
Department of Diagnostic and Interventional Radiology, Heart Center Leipzig, Strümpellstr. 39, 04289 Leipzig, Germany.
Medical Faculty, University of Leipzig, Liebigstr. 27, 04103 Leipzig, Germany.
J Clin Med. 2024 Sep 4;13(17):5247. doi: 10.3390/jcm13175247.
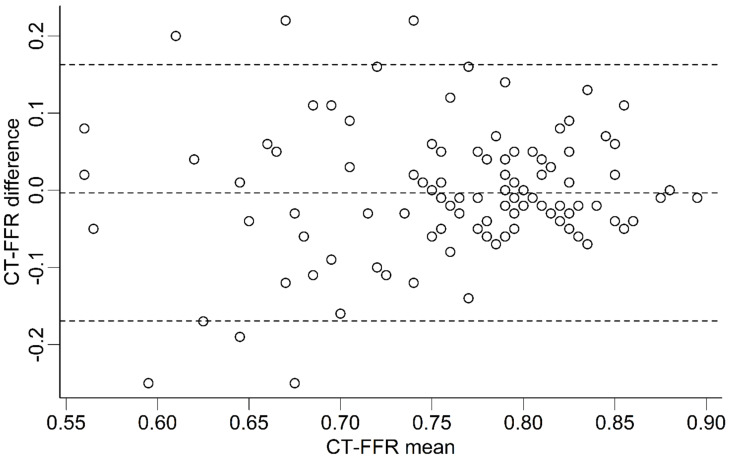
CT-derived fractional flow reserve (CT-FFR) can improve the specificity of coronary CT-angiography (cCTA) for ruling out relevant coronary artery disease (CAD) prior to transcatheter aortic valve replacement (TAVR). However, little is known about the reproducibility of CT-FFR and the influence of diffuse coronary artery calcifications or segment location. The objective was to assess the reliability of machine-learning (ML)-based CT-FFR prior to TAVR in patients without obstructive CAD and to assess the influence of image quality, coronary artery calcium score (CAC), and the location of measurement within the coronary tree. : Patients assessed for TAVR, without obstructive CAD on cCTA were evaluated with ML-based CT-FFR by two observers with differing experience. Differences in absolute values and categorization into hemodynamically relevant CAD (CT-FFR ≤ 0.80) were compared. Results in regard to CAD were also compared against invasive coronary angiography. The influence of segment location, image quality, and CAC was evaluated. : Of the screened patients, 109/388 patients did not have obstructive CAD on cCTA and were included. The median (interquartile range) difference of CT-FFR values was -0.005 (-0.09 to 0.04) ( = 0.47). Differences were smaller with high values. Recategorizations were more frequent in distal segments. Diagnostic accuracy of CT-FFR between both observers was comparable (proximal: Δ0.2%; distal: Δ0.5%) but was lower in distal segments (proximal: 98.9%/99.1%; distal: 81.1%/81.6%). Image quality and CAC had no clinically relevant influence on CT-FFR. : ML-based CT-FFR evaluation of proximal segments was more reliable. Distal segments with CT-FFR values close to the given threshold were prone to recategorization, even if absolute differences between observers were minimal and independent of image quality or CAC.
计算机断层扫描衍生的血流储备分数(CT-FFR)可提高冠状动脉计算机断层扫描血管造影(cCTA)在经导管主动脉瓣置换术(TAVR)前排除相关冠状动脉疾病(CAD)的特异性。然而,关于CT-FFR的可重复性以及弥漫性冠状动脉钙化或节段位置的影响知之甚少。目的是评估在无阻塞性CAD的患者中,基于机器学习(ML)的CT-FFR在TAVR前的可靠性,并评估图像质量、冠状动脉钙化评分(CAC)以及冠状动脉树内测量位置的影响。:对接受TAVR评估且cCTA上无阻塞性CAD的患者,由两名经验不同的观察者采用基于ML的CT-FFR进行评估。比较绝对值差异以及分类为血流动力学相关CAD(CT-FFR≤0.80)的情况。关于CAD的结果也与有创冠状动脉造影进行比较。评估节段位置、图像质量和CAC的影响。:在筛选的患者中,109/388例患者cCTA上无阻塞性CAD并被纳入。CT-FFR值的中位数(四分位间距)差异为-0.005(-0.09至0.04)(P = 0.47)。高值时差异较小。远端节段的重新分类更频繁。两名观察者之间CT-FFR的诊断准确性相当(近端:Δ0.2%;远端:Δ0.5%),但远端节段较低(近端:98.9%/99.1%;远端:81.1%/81.6%)。图像质量和CAC对CT-FFR无临床相关影响。:基于ML的近端节段CT-FFR评估更可靠。CT-FFR值接近给定阈值的远端节段容易重新分类,即使观察者之间的绝对差异最小且与图像质量或CAC无关。