Basilicata Pascale, Pieri Maria, Simonelli Angela, Capasso Emanuele, Casella Claudia, Noto Tina, Policino Fabio, Di Lorenzo Pierpaolo
Department of Advanced Biomedical Science-Legal Medicine Section, University of Naples "Federico II", 80138 Naples, Italy.
Department of Forensic and Forensic Medicine, University of Murcia, 30100 Murcia, Spain.
Toxics. 2022 Mar 30;10(4):166. doi: 10.3390/toxics10040166.
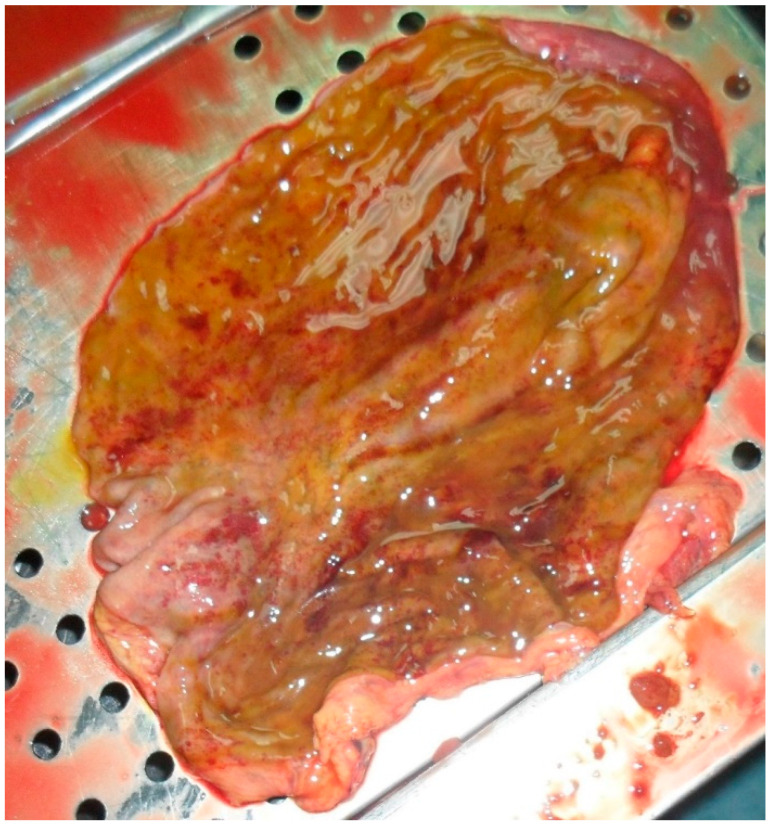
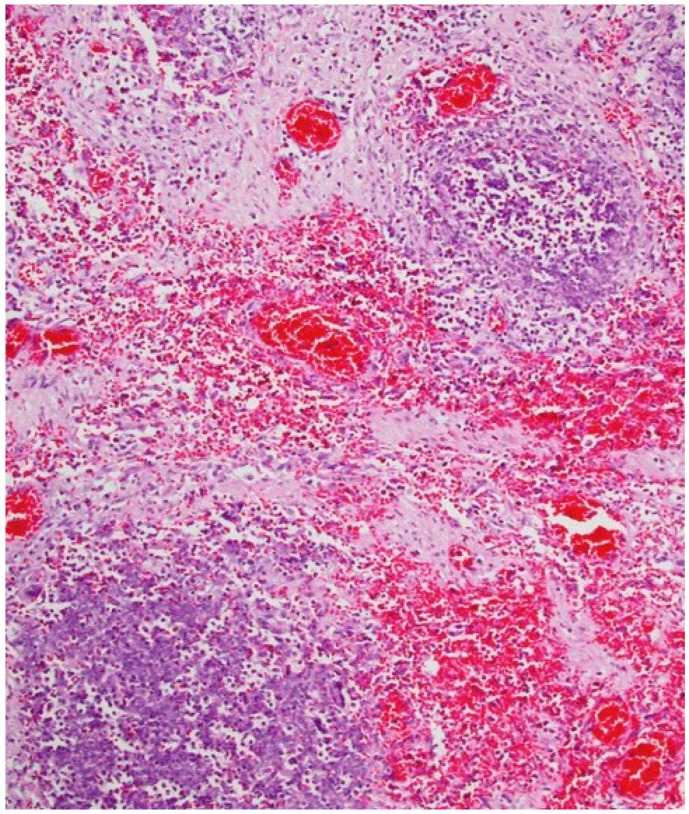
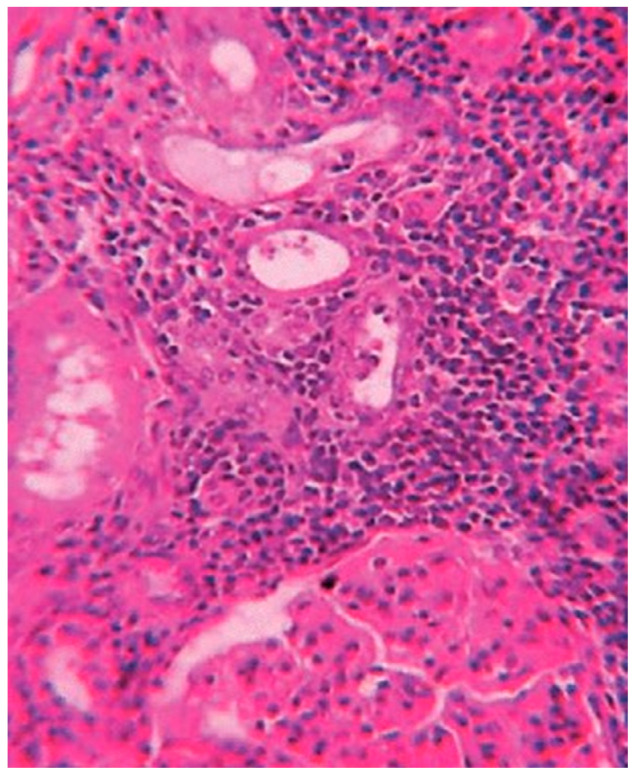
Acute chemical intoxication represents one of the major causes of Emergency Room admittance, and possible errors in diagnosis are extremely frequent, especially when patients present generic and non-specific symptoms. Diquat, a bipyridyl class of herbicides, exerts high intrinsic toxicity as a consequence of free oxygen radicals, leading to cellular death and organ dysfunctions. Following ingestion, with the major source of absorption for suicidal purposes, the chemical induces local irritating effects; systemic symptoms appear later, while specific symptoms can occur in the following 48 h. A smoker and hypertensive 50-year-old man arrives at the E.R., reporting that an episode of herbicide inhalation occurred few hours earlier. Physical examination evidenced alkalosis with hypoxemia, leucocytosis, mild hyperglycaemia and moderate increase in creatine kinase and myoglobin. Despite blood creatine kinase and myoglobin values that were higher than normal, he was prescribed with hydration and anti-pain therapy. During the night, the man left the hospital; he returned the next morning at 8:45 a.m., with cardiorespiratory arrest, medium fixed non-reactive mydriasis, diffused cyanosis of the skin and of the mucous membranes, as well as imperceptible pulse and peripheral pressure. Despite resuscitation attempts, the patient died at 9:30 a.m.; the body was immediately transferred to the morgue. Autopsy and toxicological analyses were carried out nine days later, evidencing paraquat ingestion for suicidal purposes. GC/MS analyses to verify the presence of diquat were performed on body fluids and gastric and colon contents; all specimens resulted positive, thus confirming the cause of death as herbicide ingestion (blood diquat concentration of 1.2 mg/L; more than twice the minimum to observe a systemic poisoning). The procedure followed for patient management resulted to be not in line with the provisions of both guidelines and good clinical practices. Staff did not perform clinical-diagnostical monitoring of the patient's condition or ask for more specific analyses (i.e., serum creatine phosphokinase monitoring). This misconduct led to a decrease in the patient's chances to survive.
急性化学中毒是急诊室收治的主要原因之一,诊断中可能出现的错误极为常见,尤其是当患者表现出一般的非特异性症状时。敌草快是一种联吡啶类除草剂,由于自由基的作用具有很高的内在毒性,会导致细胞死亡和器官功能障碍。摄入后(主要是因自杀目的吸收),这种化学物质会引起局部刺激作用;全身症状随后出现,而特定症状可能在接下来的48小时内出现。一名50岁的吸烟且患有高血压的男性来到急诊室,报告称几小时前发生了除草剂吸入事件。体格检查发现有碱中毒伴低氧血症、白细胞增多、轻度高血糖以及肌酸激酶和肌红蛋白中度升高。尽管血液中的肌酸激酶和肌红蛋白值高于正常水平,但他仅接受了补液和止痛治疗。当晚,该男子离开了医院;第二天上午8:45他返回医院,出现心跳呼吸骤停、中度固定性无反应性瞳孔散大、皮肤和黏膜弥漫性发绀,以及无法察觉的脉搏和外周血压。尽管进行了复苏尝试,但患者于上午9:30死亡;尸体立即被送往停尸房。九天后进行了尸检和毒理学分析,证实患者因自杀目的摄入了百草枯。对体液、胃内容物和结肠内容物进行了气相色谱/质谱分析以验证敌草快的存在;所有标本结果均为阳性,从而确认死亡原因是除草剂摄入(血液中敌草快浓度为1.2毫克/升;超过观察到全身中毒的最低浓度两倍多)。对该患者的处理程序不符合指南和良好临床实践的规定。医护人员未对患者病情进行临床诊断监测,也未要求进行更具体的分析(即血清肌酸磷酸激酶监测)。这种不当行为降低了患者的生存几率。