Aravind Gayatri, Bashir Kainat, Cameron Jill I, Howe Jo-Anne, Jaglal Susan B, Bayley Mark T, Teasell Robert W, Moineddin Rahim, Zee Joanne, Wodchis Walter P, Tee Alda, Hunter Susan, Salbach Nancy M
Department of Physical Therapy, University of Toronto, 160-500 University Avenue, Toronto, ON, M5G 1V7, Canada.
Department of Occupational Science and Occupational Therapy, University of Toronto, 160-500 University Avenue, Toronto, ON, M5G 1V7, Canada.
Pilot Feasibility Stud. 2022 Apr 22;8(1):88. doi: 10.1186/s40814-022-01037-9.
Despite the potential for community-based exercise programs supported through healthcare-community partnerships (CBEP-HCPs) to improve function post-stroke, insufficient trial evidence limits widespread program implementation and funding. We evaluated the feasibility and acceptability of a CBEP-HCP compared to a waitlist control group to improve everyday function among people post-stroke.
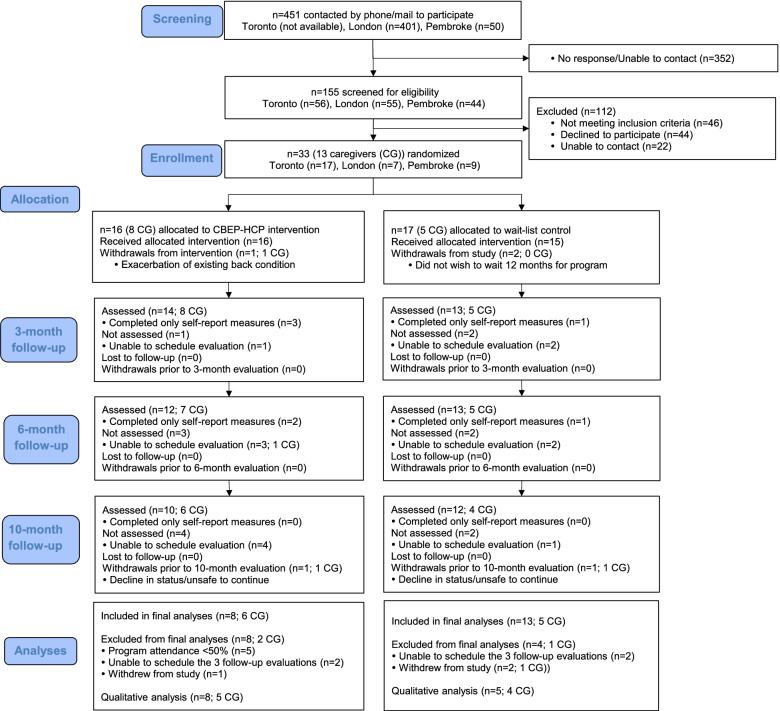
We conducted a 3-site, pilot randomized trial with blinded follow-up evaluations at 3, 6, and 10 months. Community-dwelling adults able to walk 10 m were stratified by site and gait speed and randomized (1:1) to a CBEP-HCP or waitlist control group. The CBEP-HCP involved a 1-h, group exercise class, with repetitive and progressive practice of functional balance and mobility tasks, twice a week for 12 weeks. We offered the exercise program to the waitlist group at 10 months. We interviewed 13 participants and 9 caregivers post-intervention and triangulated quantitative and qualitative results. Study outcomes included feasibility of recruitment, interventions, retention, and data collection, and potential effect on everyday function.
Thirty-three people with stroke were randomized to the intervention (n = 16) or waitlist group (n = 17). We recruited 1-2 participants/month at each site. Participants preferred being recruited by a familiar healthcare professional. Participants described a 10- or 12-month wait in the control group as too long. The exercise program was implemented per protocol across sites. Five participants (31%) in the intervention group attended fewer than 50% of classes for health reasons. In the intervention and waitlist group, retention was 88% and 82%, respectively, and attendance at 10-month evaluations was 63% and 71%, respectively. Participants described inclement weather, availability of transportation, and long commutes as barriers to attending exercise classes and evaluations. Among participants in the CBEP-HCP who attended ≥ 50% of classes, quantitative and qualitative results suggested an immediate effect of the intervention on balance, balance self-efficacy, lower limb strength, everyday function, and overall health.
The CBEP-HCP appears feasible and potentially beneficial. Findings will inform protocol revisions to optimize recruitment, and program and evaluation attendance in a future trial.
ClinicalTrials.gov , NCT03122626 . Registered April 21, 2017 - retrospectively registered.
尽管通过医疗保健与社区伙伴关系支持的社区锻炼计划(CBEP - HCP)有潜力改善中风后的功能,但试验证据不足限制了该计划的广泛实施和资金投入。我们评估了与等待名单对照组相比,CBEP - HCP改善中风患者日常功能的可行性和可接受性。
我们进行了一项在3个地点开展的试点随机试验,并在3个月、6个月和10个月时进行盲法随访评估。能够行走10米的社区居住成年人按地点和步态速度分层,随机(1:1)分为CBEP - HCP组或等待名单对照组。CBEP - HCP包括一节1小时的团体锻炼课程,对功能性平衡和移动任务进行重复和渐进式练习,每周两次,共12周。我们在10个月时为等待名单组提供该锻炼计划。干预后,我们对13名参与者和9名护理人员进行了访谈,并对定量和定性结果进行了三角验证。研究结果包括招募、干预、留存和数据收集的可行性,以及对日常功能的潜在影响。
33名中风患者被随机分为干预组(n = 16)或等待名单组(n = 17)。每个地点每月招募1 - 2名参与者。参与者更喜欢由熟悉的医疗保健专业人员招募。参与者表示,对照组10个月或12个月的等待时间太长。锻炼计划在各地点均按方案实施。干预组中有5名参与者(31%)因健康原因参加的课程少于50%。在干预组和等待名单组中,留存率分别为88%和82%,10个月评估时的出勤率分别为63%和71%。参与者称恶劣天气、交通便利性和长途通勤是参加锻炼课程和评估的障碍。在参加了≥50%课程的CBEP - HCP参与者中,定量和定性结果表明干预对平衡、平衡自我效能、下肢力量、日常功能和整体健康有即时影响。
CBEP - HCP似乎是可行的且可能有益。研究结果将为方案修订提供参考,以优化未来试验中的招募、项目参与和评估参与情况。
ClinicalTrials.gov,NCT03122626。2017年4月21日注册 - 追溯注册。