Signal Transduction and Molecular Hematology, Ludwig Institute for Cancer Research, Brussels, Belgium.
Signal Transduction on Molecular Hematology, de Duve Institute, Université Catholique de Louvain, Bruxelles, Belgium.
J Immunother Cancer. 2022 Apr;10(4). doi: 10.1136/jitc-2021-002838.
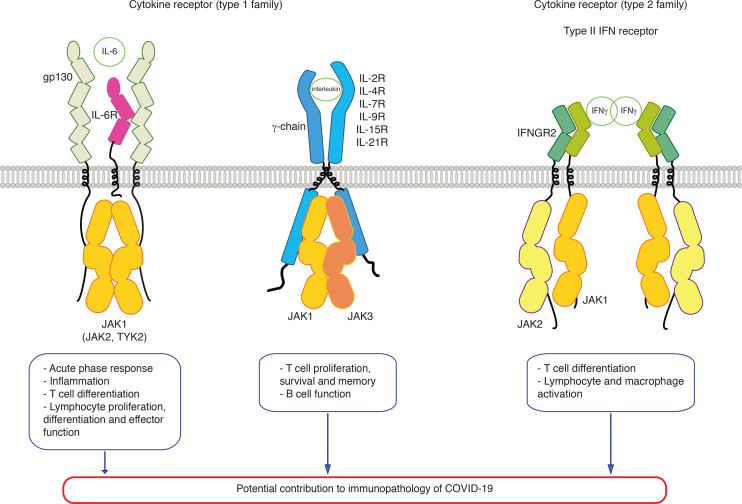
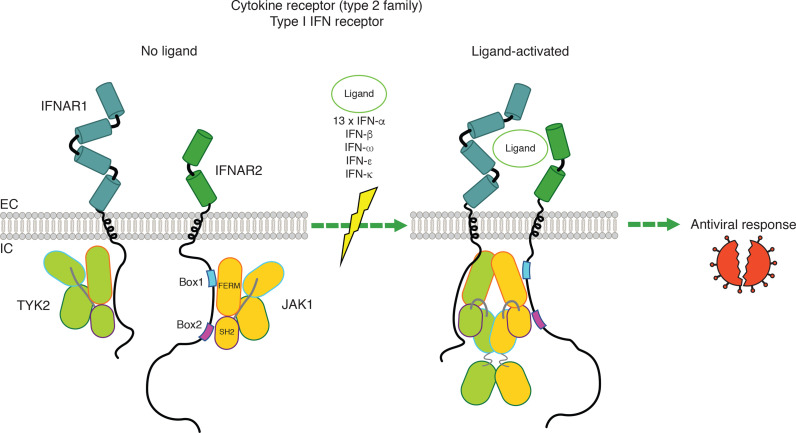
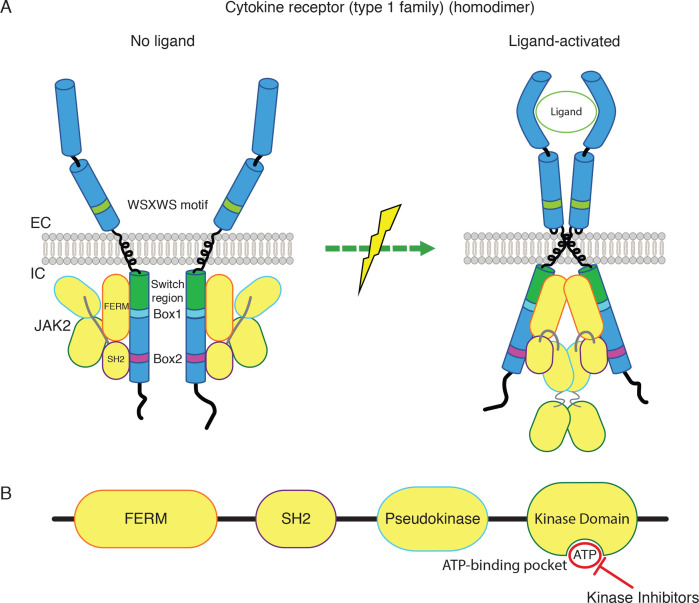
During SARS-CoV-2 infection, the innate immune response can be inhibited or delayed, and the subsequent persistent viral replication can induce emergency signals that may culminate in a cytokine storm contributing to the severe evolution of COVID-19. Cytokines are key regulators of the immune response and virus clearance, and, as such, are linked to the-possibly altered-response to the SARS-CoV-2. They act via a family of more than 40 transmembrane receptors that are coupled to one or several of the 4 Janus kinases (JAKs) coded by the human genome, namely JAK1, JAK2, JAK3, and TYK2. Once activated, JAKs act on pathways for either survival, proliferation, differentiation, immune regulation or, in the case of type I interferons, antiviral and antiproliferative effects. Studies of graft-versus-host and systemic rheumatic diseases indicated that JAK inhibitors (JAKi) exert immunosuppressive effects that are non-redundant with those of corticotherapy. Therefore, they hold the potential to cut-off pathological reactions in COVID-19. Significant clinical experience already exists with several JAKi in COVID-19, such as baricitinib, ruxolitinib, tofacitinib, and nezulcitinib, which were suggested by a meta-analysis (Patoulias ) to exert a benefit in terms of risk reduction concerning major outcomes when added to standard of care in patients with COVID-19. Yet, only baricitinib is recommended in first line for severe COVID-19 treatment by the WHO, as it is the only JAKi that has proven efficient to reduce mortality in individual randomized clinical trials (RCT), especially the Adaptive COVID-19 Treatment Trial (ACTT-2) and COV-BARRIER phase 3 trials. As for secondary effects of JAKi treatment, the main caution with baricitinib consists in the induced immunosuppression as long-term side effects should not be an issue in patients treated for COVID-19.We discuss whether a class effect of JAKi may be emerging in COVID-19 treatment, although at the moment the convincing data are for baricitinib only. Given the key role of JAK1 in both type I IFN action and signaling by cytokines involved in pathogenic effects, establishing the precise timing of treatment will be very important in future trials, along with the control of viral replication by associating antiviral molecules.
在 SARS-CoV-2 感染期间,先天免疫反应可能会受到抑制或延迟,随后持续的病毒复制会引发紧急信号,导致细胞因子风暴,从而导致 COVID-19 的严重恶化。细胞因子是免疫反应和病毒清除的关键调节剂,因此与 SARS-CoV-2 的反应改变有关。它们通过一个由超过 40 种跨膜受体组成的家族发挥作用,这些受体与人类基因组编码的 4 种 Janus 激酶(JAK)中的一种或几种偶联,即 JAK1、JAK2、JAK3 和 TYK2。一旦被激活,JAK 就会作用于生存、增殖、分化、免疫调节的途径,或者在 I 型干扰素的情况下,发挥抗病毒和抗增殖作用。移植物抗宿主病和系统性风湿病的研究表明,JAK 抑制剂(JAKi)具有非皮质激素治疗的免疫抑制作用。因此,它们有可能阻断 COVID-19 的病理反应。目前已经有几种 JAKi 在 COVID-19 中得到了显著的临床应用,如巴利昔替尼、鲁索利替尼、托法替尼和奈泽替尼,荟萃分析(Patoulias)表明,在 COVID-19 患者的标准治疗中加入这些药物可以降低主要结局的风险。然而,只有巴利昔替尼被世界卫生组织推荐用于 COVID-19 的一线治疗,因为它是唯一一种在个体随机临床试验(RCT)中被证明能降低死亡率的 JAKi,特别是适应性 COVID-19 治疗试验(ACTT-2)和 COV-BARRIER 三期试验。至于 JAKi 治疗的次要影响,巴利昔替尼的主要注意事项是诱导免疫抑制,因为长期的副作用不应成为 COVID-19 患者治疗的问题。我们讨论了 JAKi 在 COVID-19 治疗中是否可能出现类效应,尽管目前令人信服的数据仅适用于巴利昔替尼。鉴于 JAK1 在 I 型干扰素作用和细胞因子信号通路中的关键作用,以及细胞因子在致病作用中的信号通路,确定治疗的精确时间将是未来试验的关键,同时还需要通过联合抗病毒分子来控制病毒复制。