Optum, 1325 Boylston Street, 11th Floor, Boston, MA, 02215, USA.
IQVIA, Plymouth Meeting, PA, USA.
BMC Infect Dis. 2022 Apr 29;22(1):413. doi: 10.1186/s12879-022-07383-6.
There are limited data on risk factors for serious outcomes and death from COVID-19 among patients representative of the U.S.
The objective of this study was to determine risk factors for critical care, ventilation, and death among hospitalized patients with COVID-19.
This was a cohort study using data from Optum's longitudinal COVID-19 electronic health record database derived from a network of healthcare provider organizations across the US. The study included patients with confirmed COVID-19 (presence of ICD-10-CM code U07.1 and/or positive SARS-CoV-2 test) between January 2020 and November 2020. Patient characteristics and clinical variables at start of hospitalization were evaluated for their association with subsequent serious outcomes (critical care, mechanical ventilation, and death) using odds ratios (OR) and 95% confidence intervals (CI) from logistic regression, adjusted for demographic variables.
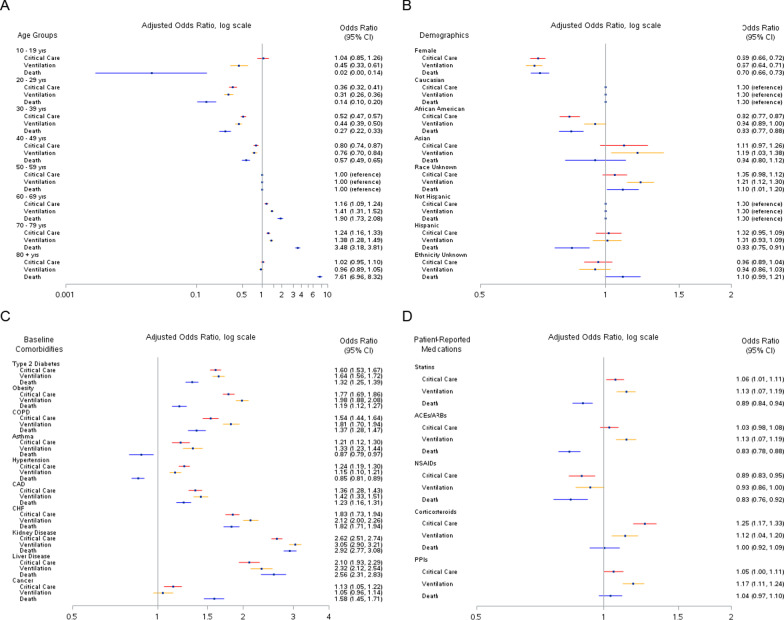
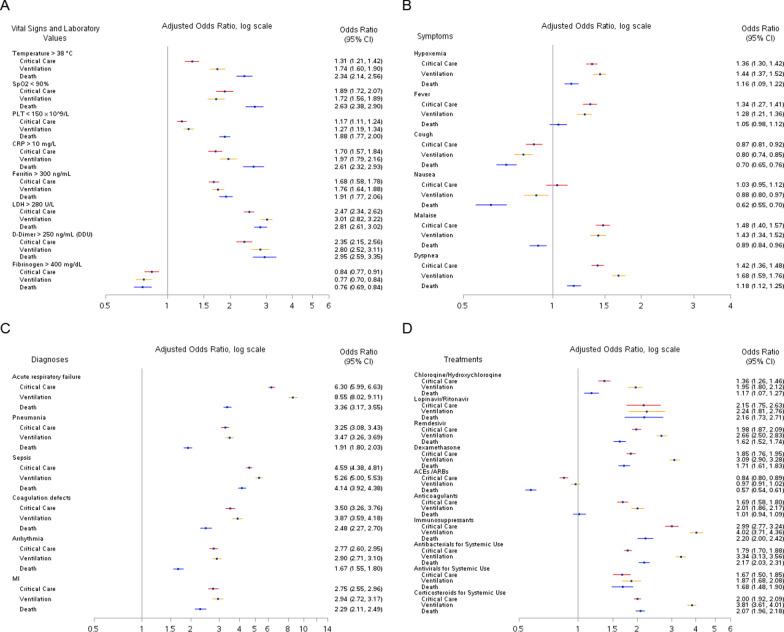
Among 56,996 hospitalized COVID-19 patients (49.5% male and 72.4% ≥ 50 years), 11,967 received critical care, 9136 received mechanical ventilation, and 8526 died. The median duration of hospitalization was 6 days (IQR: 4, 11), and this was longer among patients that experienced an outcome: 11 days (IQR: 6, 19) for critical care, 15 days (IQR: 8, 24) for mechanical ventilation, and 10 days (IQR: 5, 17) for death. Dyspnea and hypoxemia were the most prevalent symptoms and both were associated with serious outcomes in adjusted models. Additionally, temperature, C-reactive protein, ferritin, lactate dehydrogenase, D-dimer, and oxygen saturation measured during hospitalization were predictors of serious outcomes as were several in-hospital diagnoses. The strongest associations were observed for acute respiratory failure (critical care: OR, 6.30; 95% CI, 5.99-6.63; ventilation: OR, 8.55; 95% CI, 8.02-9.11; death: OR, 3.36; 95% CI, 3.17-3.55) and sepsis (critical care: OR, 4.59; 95% CI, 4.39-4.81; ventilation: OR, 5.26; 95% CI, 5.00-5.53; death: OR, 4.14; 95% CI, 3.92-4.38). Treatment with angiotensin-converting enzyme inhibitors/angiotensin receptor blockers during hospitalization were inversely associated with death (OR, 0.57; 95% CI, 0.54-0.61).
We identified several clinical characteristics associated with receipt of critical care, mechanical ventilation, and death among COVID-19 patients. Future studies into the mechanisms that lead to severe COVID-19 disease are warranted.
在美国代表性人群中,关于 COVID-19 严重结局和死亡的风险因素数据有限。
本研究的目的是确定住院 COVID-19 患者发生重症监护、通气和死亡的风险因素。
这是一项队列研究,使用了来自 Optum 的 COVID-19 电子健康记录数据库的数据,该数据库来自美国医疗保健提供者组织网络。研究包括 2020 年 1 月至 2020 年 11 月期间确诊为 COVID-19 的患者(存在 ICD-10-CM 代码 U07.1 和/或 SARS-CoV-2 检测阳性)。使用逻辑回归分析患者入院时的特征和临床变量与随后的严重结局(重症监护、机械通气和死亡)之间的关联,使用比值比(OR)和 95%置信区间(CI),并调整了人口统计学变量。
在 56996 例住院 COVID-19 患者中(49.5%为男性,72.4%≥50 岁),11967 例接受了重症监护,9136 例接受了机械通气,8526 例死亡。住院中位数为 6 天(IQR:4,11),经历结局的患者住院时间更长:重症监护 11 天(IQR:6,19),机械通气 15 天(IQR:8,24),死亡 10 天(IQR:5,17)。呼吸困难和低氧血症是最常见的症状,在调整后的模型中均与严重结局相关。此外,住院期间测量的体温、C 反应蛋白、铁蛋白、乳酸脱氢酶、D-二聚体和氧饱和度以及几种院内诊断也是严重结局的预测因素。最强的关联见于急性呼吸衰竭(重症监护:OR,6.30;95%CI,5.99-6.63;通气:OR,8.55;95%CI,8.02-9.11;死亡:OR,3.36;95%CI,3.17-3.55)和败血症(重症监护:OR,4.59;95%CI,4.39-4.81;通气:OR,5.26;95%CI,5.00-5.53;死亡:OR,4.14;95%CI,3.92-4.38)。住院期间使用血管紧张素转换酶抑制剂/血管紧张素受体阻滞剂与死亡呈负相关(OR,0.57;95%CI,0.54-0.61)。
我们确定了与 COVID-19 患者接受重症监护、机械通气和死亡相关的几个临床特征。有必要对导致严重 COVID-19 疾病的机制进行进一步研究。