Departments of Epidemiology and Radiology, Erasmus University Medical Center, Rotterdam, The Netherlands.
Department of Population Medicine, Harvard Medical School and Harvard Pilgrim Health Care Institute, Boston, MA, USA; Cancer Outcomes, Public Policy, and Effectiveness Research Center, Yale University School of Medicine, New Haven, CT, USA.
Value Health. 2022 Aug;25(8):1268-1280. doi: 10.1016/j.jval.2022.03.016. Epub 2022 Apr 28.
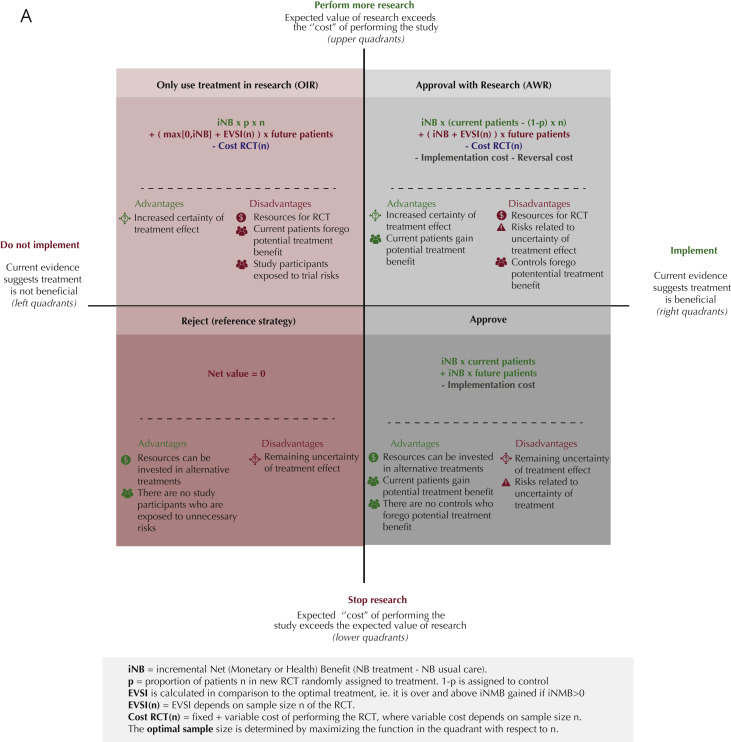
The COVID-19 pandemic necessitates time-sensitive policy and implementation decisions regarding new therapies in the face of uncertainty. This study aimed to quantify consequences of approving therapies or pursuing further research: immediate approval, use only in research, approval with research (eg, emergency use authorization), or reject.
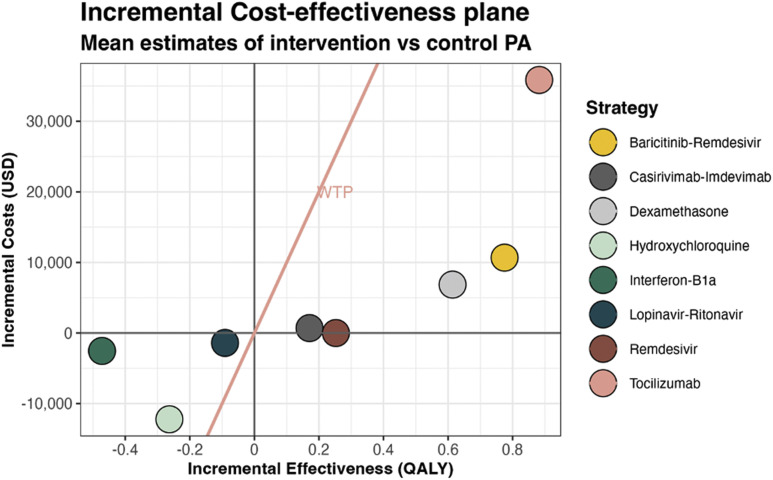
Using a cohort state-transition model for hospitalized patients with COVID-19, we estimated quality-adjusted life-years (QALYs) and costs associated with the following interventions: hydroxychloroquine, remdesivir, casirivimab-imdevimab, dexamethasone, baricitinib-remdesivir, tocilizumab, lopinavir-ritonavir, interferon beta-1a, and usual care. We used the model outcomes to conduct cost-effectiveness and value of information analyses from a US healthcare perspective and a lifetime horizon.
Assuming a $100 000-per-QALY willingness-to-pay threshold, only remdesivir, casirivimab-imdevimab, dexamethasone, baricitinib-remdesivir, and tocilizumab were (cost-) effective (incremental net health benefit 0.252, 0.164, 0.545, 0.668, and 0.524 QALYs and incremental net monetary benefit $25 249, $16 375, $54 526, $66 826, and $52 378). Our value of information analyses suggest that most value can be obtained if these 5 therapies are approved for immediate use rather than requiring additional randomized controlled trials (RCTs) (net value $20.6 billion, $13.4 billion, $7.4 billion, $54.6 billion, and $7.1 billion), hydroxychloroquine (net value $198 million) is only used in further RCTs if seeking to demonstrate decremental cost-effectiveness and otherwise rejected, and interferon beta-1a and lopinavir-ritonavir are rejected (ie, neither approved nor additional RCTs).
Estimating the real-time value of collecting additional evidence during the pandemic can inform policy makers and clinicians about the optimal moment to implement therapies and whether to perform further research.
面对不确定性,新冠疫情大流行需要针对新疗法做出及时的政策和实施决策。本研究旨在量化批准疗法或开展进一步研究的后果:立即批准、仅用于研究、批准并开展研究(例如,紧急使用授权)或拒绝。
我们使用针对 COVID-19 住院患者的队列状态转换模型,估算了以下干预措施相关的质量调整生命年(QALY)和成本:羟氯喹、瑞德西韦、卡司瑞韦单抗-伊德韦单抗、地塞米松、巴瑞替尼-瑞德西韦、托珠单抗、洛匹那韦-利托那韦、干扰素β-1a 和常规治疗。我们使用模型结果,从美国医疗保健角度和终生时间范围,进行成本效益和信息价值分析。
假设 10 万美元/QALY 的意愿支付阈值,只有瑞德西韦、卡司瑞韦单抗-伊德韦单抗、地塞米松、巴瑞替尼-瑞德西韦和托珠单抗具有成本效益(增量净健康收益分别为 0.252、0.164、0.545、0.668 和 0.524 QALY 和增量净货币收益分别为 25249 美元、16375 美元、54526 美元、66826 美元和 52378 美元)。我们的信息价值分析表明,如果这 5 种疗法立即批准使用,而不是需要进行更多的随机对照试验(RCT),则可以获得大部分价值(净价值分别为 206 亿美元、134 亿美元、74 亿美元、546 亿美元和 71 亿美元),羟氯喹(净价值 1.98 亿美元)只有在寻求证明成本效益递减时才会进行进一步的 RCT,否则会被拒绝,而干扰素β-1a 和洛匹那韦-利托那韦则被拒绝(即不批准也不开展进一步的 RCT)。
实时估计在大流行期间收集额外证据的价值,可以为决策者和临床医生提供有关何时实施疗法以及是否开展进一步研究的最佳时机的信息。