Hospices Civils de Lyon, Département des maladies infectieuses et tropicales, F-69004, Lyon, France; Centre International de Recherche en Infectiologie (CIRI), Inserm 1111, Université Claude Bernard Lyon 1, CNRS, UMR5308, École Normale Supérieure de Lyon, Univ Lyon, F-69007, Lyon, France.
Université de Paris, IAME, INSERM, F-75018 Paris, France; AP-HP, Hôpital Bichat, Service de maladies infectieuses et tropicales, F-75018 Paris, France; National Institute for Health Research, Health Protection Research Unit in Healthcare Associated Infections and Antimicrobial Resistance, Imperial College London, London, UK.
Clin Microbiol Infect. 2021 Dec;27(12):1826-1837. doi: 10.1016/j.cmi.2021.05.020. Epub 2021 May 26.
We evaluated the clinical, virological and safety outcomes of lopinavir/ritonavir, lopinavir/ritonavir-interferon (IFN)-β-1a, hydroxychloroquine or remdesivir in comparison to standard of care (control) in coronavirus 2019 disease (COVID-19) inpatients requiring oxygen and/or ventilatory support.
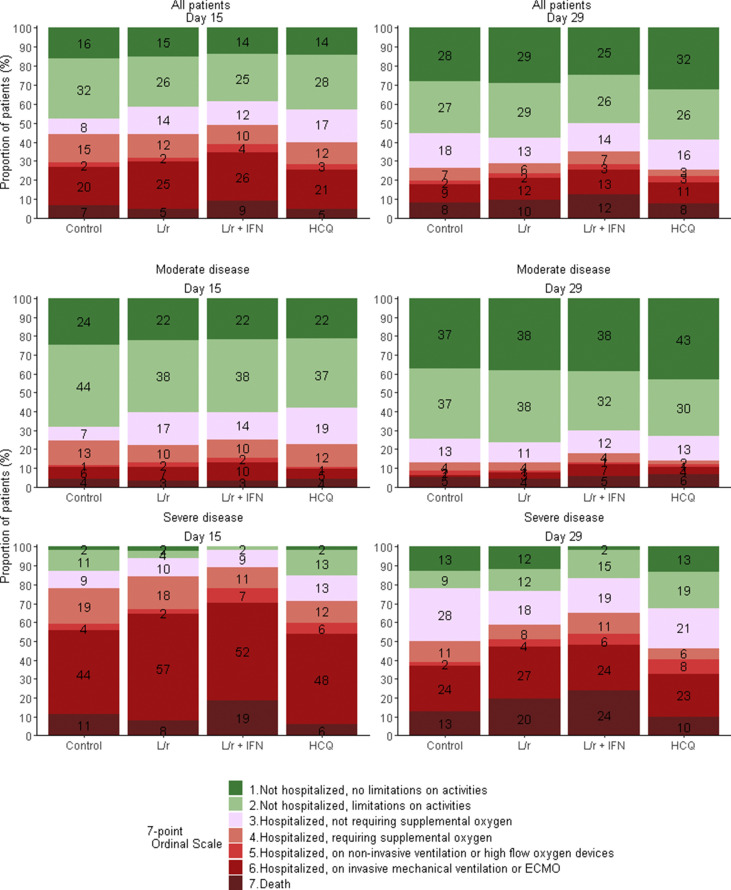
We conducted a phase III multicentre, open-label, randomized 1:1:1:1:1, adaptive, controlled trial (DisCoVeRy), an add-on to the Solidarity trial (NCT04315948, EudraCT2020-000936-23). The primary outcome was the clinical status at day 15, measured by the WHO seven-point ordinal scale. Secondary outcomes included quantification of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in respiratory specimens and pharmacokinetic and safety analyses. We report the results for the lopinavir/ritonavir-containing arms and for the hydroxychloroquine arm, trials of which were stopped prematurely.
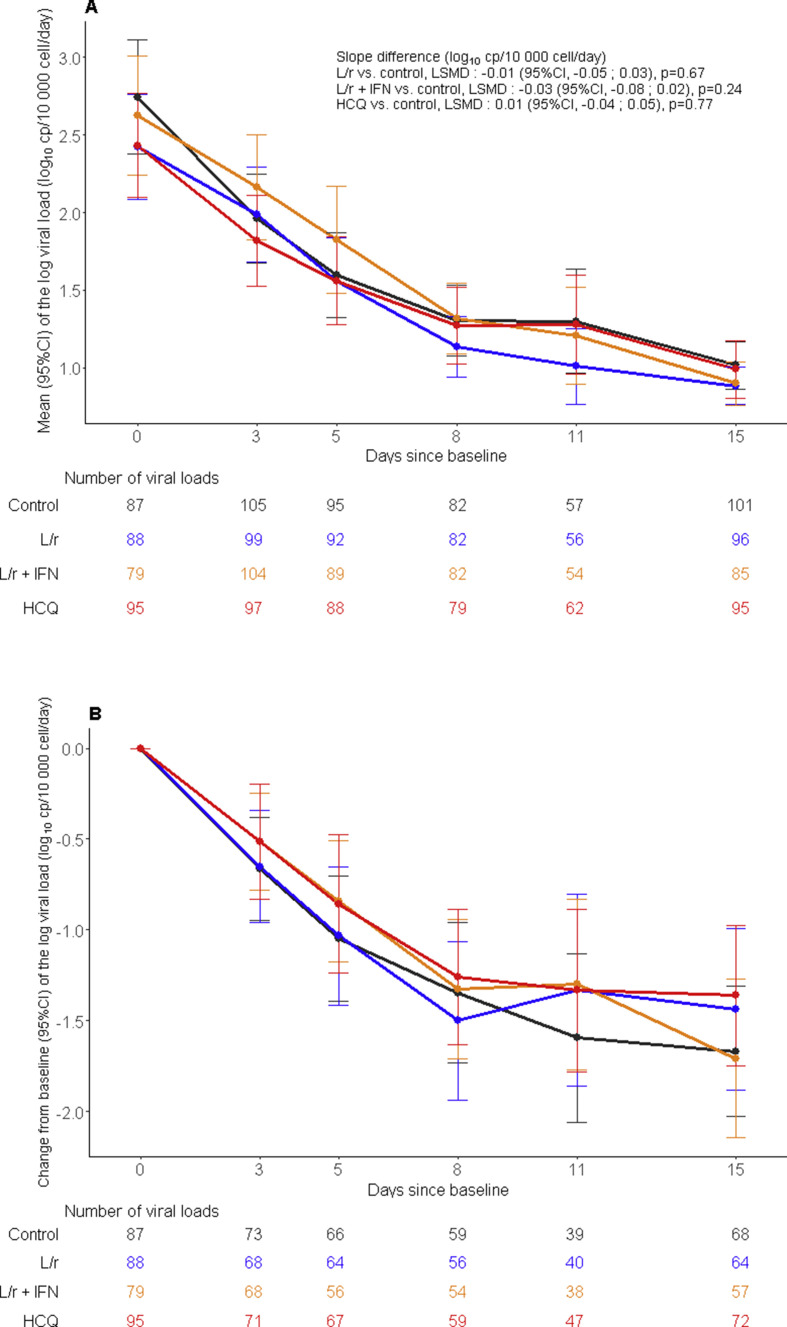
The intention-to-treat population included 583 participants-lopinavir/ritonavir (n = 145), lopinavir/ritonavir-IFN-β-1a (n = 145), hydroxychloroquine (n = 145), control (n = 148)-among whom 418 (71.7%) were male, the median age was 63 years (IQR 54-71), and 211 (36.2%) had a severe disease. The day-15 clinical status was not improved with the investigational treatments: lopinavir/ritonavir versus control, adjusted odds ratio (aOR) 0.83, (95% confidence interval (CI) 0.55-1.26, p 0.39), lopinavir/ritonavir-IFN-β-1a versus control, aOR 0.69 (95%CI 0.45-1.04, p 0.08), and hydroxychloroquine versus control, aOR 0.93 (95%CI 0.62-1.41, p 0.75). No significant effect of investigational treatment was observed on SARS-CoV-2 clearance. Trough plasma concentrations of lopinavir and ritonavir were higher than those expected, while those of hydroxychloroquine were those expected with the dosing regimen. The occurrence of serious adverse events was significantly higher in participants allocated to the lopinavir/ritonavir-containing arms.
In adults hospitalized for COVID-19, lopinavir/ritonavir, lopinavir/ritonavir-IFN-β-1a and hydroxychloroquine improved neither the clinical status at day 15 nor SARS-CoV-2 clearance in respiratory tract specimens.
我们评估了洛匹那韦/利托那韦、洛匹那韦/利托那韦-干扰素 (IFN)-β-1a、羟氯喹或瑞德西韦在需要氧疗和/或通气支持的 2019 年冠状病毒病 (COVID-19) 住院患者中的临床、病毒学和安全性结局,与标准治疗 (对照) 相比。
我们开展了一项 III 期、多中心、开放性标签、随机 1:1:1:1:1、适应性、对照试验 (DisCoVeRy),是 Solidarity 试验 (NCT04315948,EudraCT2020-000936-23) 的附加研究。主要结局是第 15 天的临床状态,采用世界卫生组织 (WHO) 7 点等级量表进行评估。次要结局包括呼吸道标本中严重急性呼吸综合征冠状病毒 2 (SARS-CoV-2) 的定量和药代动力学及安全性分析。我们报告洛匹那韦/利托那韦组和羟氯喹组的结果,这两组试验均提前终止。
意向治疗人群包括 583 例参与者-洛匹那韦/利托那韦 (n=145)、洛匹那韦/利托那韦-IFN-β-1a (n=145)、羟氯喹 (n=145)、对照 (n=148)-其中 418 例 (71.7%) 为男性,中位年龄为 63 岁 (IQR 54-71),211 例 (36.2%) 为重症患者。与对照相比,研究治疗并未改善第 15 天的临床状态:洛匹那韦/利托那韦与对照相比,调整后比值比 (aOR) 0.83 (95%CI 0.55-1.26,p=0.39),洛匹那韦/利托那韦-IFN-β-1a 与对照相比,aOR 0.69 (95%CI 0.45-1.04,p=0.08),羟氯喹与对照相比,aOR 0.93 (95%CI 0.62-1.41,p=0.75)。未观察到研究治疗对 SARS-CoV-2 清除有显著影响。洛匹那韦和利托那韦的血药谷浓度高于预期,而羟氯喹的血药谷浓度与给药方案相符。接受洛匹那韦/利托那韦治疗的参与者发生严重不良事件的比例显著更高。
在因 COVID-19 住院的成年人中,洛匹那韦/利托那韦、洛匹那韦/利托那韦-IFN-β-1a 和羟氯喹既不能改善第 15 天的临床状态,也不能改善呼吸道标本中 SARS-CoV-2 的清除。